Commentary
George Daskalakis, Marianna Theodora, Sofia Koura, Dimitrios Loutradis, Vasilios Pergialiotis
1st department of Obstetrics and Gynecology, Alexandra Hospital, National and Kapodistrian University of Athens, Greece.
Correspondence: Vasilios Pergialiotis, MD, MSc, PhD, 6, Danaidon str., Halandri 15232 – Greece, e-mail: pergialiotis@yahoo.com
![]()
The emergence of the COVID-19 pandemic caused disruption of daily activities in almost every aspect of life1. Epidemiological reflexes were criticized by many as inadequate as the World Health Organization characterized COVID-19 as a pandemic two months after the initial reports of a cluster of cases of pneumonia in Wuhan2. In a national level governmental reflexes across the world varied significantly and countries that acted proactively effectively kept the prevalence of the disease in acceptable levels that could be handled by healthcare systems. Greece`s response to the COVID-19 pandemic was immediate as within 12 days authorities decided to suspend educational and leisure activities and within one-month non-essential movement was also restricted. Consequently, public healthcare was also restricted to emergent cases, whereas, elective cases were prioritized according to their severity, in order to ensure social distancing. To date, the majority of publications in the international literature report on morbidity, mortality rates and potential treatment strategies for the treatment of the virus. However, the impact of restrictive strategies on routine healthcare activities is scarcely reported. Pregnant women represent a subgroup of patients which has not received adequate research in this field3-4.
In our institution, which is the largest tertiary hospital involved in obstetrics and gynecology in Greece, we observed a steep decline in antenatal screening and diagnostic tests (including nuchal translucency, second and third trimester ultrasonographic screening, amniocentesis and chorionic villus sampling) after comparing cases that referred to our department between February and May 2020 and those that were handled between February and May 2019 (Figure 1). Particularly, during the period of severe restriction of daily activities (April, early May) the number of appointments for antenatal screening dropped to zero. In contrast, comparable numbers of admission were observed in the high-risk pregnancy department (Figure 2).
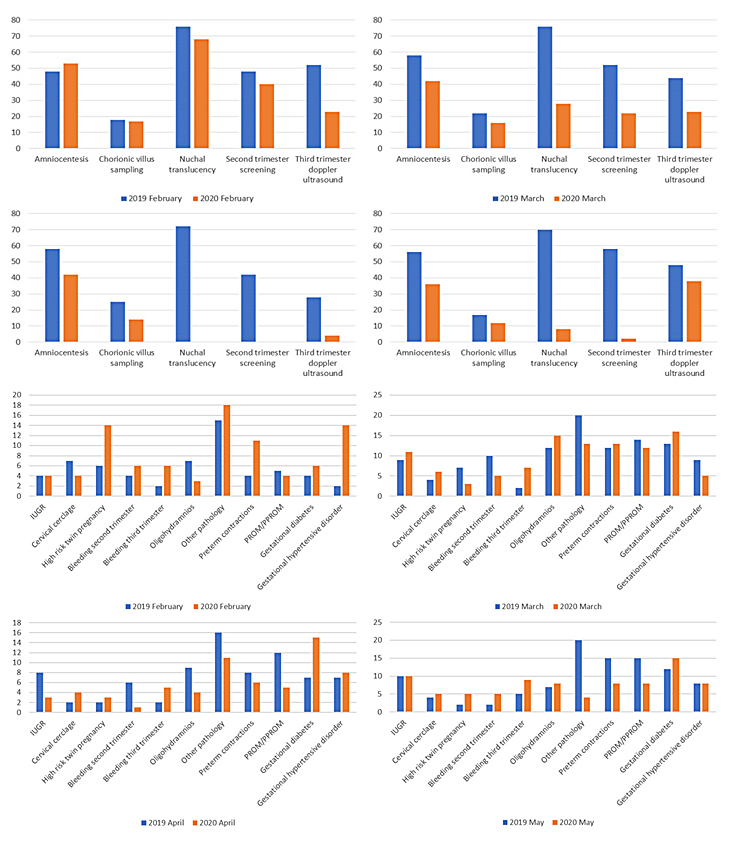
Figure 1. Comparative analysis of performed screening tests and cases admitted for pregnancy complications between 2019 (blue lines) and 2020 (orange lines).
Taking into consideration the importance of antenatal care it is easily understandable that further research is needed in this field, in order to ensure that pregnant women do not receive sub-optimal healthcare following the imposition of restrictive measures. To date, many national societies recommend reduction of the usual antenatal visits 5,6. However, we have to establish a structured plan of routine healthcare during this pandemic, in order to prevent a no visit at all practice. Given the possibility of a second wave of COVID-197 it becomes reasonable to implement international policies as well as national healthcare strategies that will help prevent the emergence of a new pandemic without compromising routine patient healthcare.
Disclosure
The authors report no conflict of interest.
Funding
None to disclose for all authors.
References
1. Elangovan S, Mahrous A, Marchini L. Disruptions during a pandemic: Gaps identified and lessons learned. J Dent Educ 2020.
2. WHO Timeline – COVID-19. World Health Organization. https://www.who.int/news-room/detail/27-04-2020-who-timeline—covid-19. Retrieved June 5, 2020.
3. Whitehead CL, Walker SP. Consider pregnancy in COVID-19 therapeutic drug and vaccine trials. Lancet 2020;395:e92.
4. Favre G, Pomar L, Musso D, Baud D. 2019-nCoV epidemic: what about pregnancies? Lancet 2020;395:e40.
5. Royal College of Obstetricians & Gynaecologists. Coronavirus infection and pregnancy. Information for healthcare professionals. Version 9: Published Wednesday 13 May 2020.
6. Poon LC, Yang H, Lee JCS, et al. ISUOG Interim Guidance on 2019 novel coronavirus infection during pregnancy and puerperium: information for healthcare professionals. Ultrasound in Obstetrics & Gynecology 2020;55:700-8.
7. Xu S, Li Y. Beware of the second wave of COVID-19. Lancet 2020;395:1321-2.