Research
HJOG 2026, 25 (2), 82-89| doi: 10.33574/hjog.0619
Elpida Salasidou1, Eirini Boureka1, Antigoni Pavlaki2, Apostolos Mamopoulos1, Themistoklis Dagklis1, Ioannis Tsakiridis1
1Third Department of Obstetrics and Gynaecology, School of Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, Thessaloniki, Greece
2Neonatal intensive care unit, Hippokrateio General Hospital of Thessaloniki, Greece
Correspondence: Ioannis Tsakiridis, Konstantinoupoleos 49, 54642, Thessaloniki Tel: +30 2313312120 and Fax: +30 2310 992950, e-mail: iotsakir@gmail.com
![]()
Abstract
Introduction: Neonatal intensive care units provide specialized care for infants at risk of morbidity and mortality, with prematurity remaining the leading cause of admission worldwide.
Material and Methods: This retrospective study analyzed neonates admitted to a tertiary NICU in Northern Greece between January 2022 and December 2024, examining outcomes in relation to gestational age, birthweight, cause of admission, delivery mode and feeding practices.
Results: In total, 561 neonates were included. Prematurity accounted for 48% of admissions, followed by respiratory problems (13%), while 60% of neonates were born with low birthweight, including 17% with very low birthweight. Survival improved significantly with increasing gestational age and birthweight, reaching 99.3% in term neonates and 99.6% in those ≥2500 g, but remained lower in infants born <28 weeks (70.8%) and <1000 g (67.6%) (p<0.001). Cesarean delivery was associated with improved survival in neonates <28 weeks (p=0.006), whereas feeding method at discharge was not significantly related to length of hospital stay (p=0.89). Overall, prematurity was strongly associated with lower gestational age, lower birthweight and longer hospitalization (p<0.001).
Conclusion: These findings confirm that prematurity continues to drive NICU admissions and adverse neonatal outcomes, with gestational age and birthweight as the most important predictors of survival. Cesarean delivery may confer benefits at the extreme prematurity, while feeding route at discharge does not appear to impact hospitalization duration. Targeted perinatal strategies are required to optimize survival and outcomes in extremely preterm and very low birthweight infants.
Keywords: NICU, prematurity, neonatal outcomes, birthweight, gestational age, cesarean section, feeding
Introduction
Neonatal intensive care units (NICUs) play a vital role in managing newborns with increased risk for morbidity and mortality, especially those born preterm; prematurity remains the leading cause of neonatal death globally and is associated with increased resource utilization in NICUs (1). Internationally, preterm birth rates range from 4% to 16%, and in NICUs, the majority of admissions are due to complications related to early birth (2). Respiratory distress, infections, jaundice, and feeding problems are also prevalent causes of admission (3,4).
Moreover, survival increases significantly with each additional week of gestation and each 100g gain in birthweight (5,6). Recent literature supports that cesarean section may improve survival in extremely preterm infants, though it may not be beneficial in more mature neonates (7,8). Feeding practices, particularly the early initiation of enteral nutrition and use of breast milk, also influence outcomes including length of hospital stay and weight gain (9,10).
This study aimed to investigate the perinatal outcomes of neonates admitted to NICU, focusing on causes of admission, survival, gestational age, and other relevant factors including birthweight, feeding type and delivery mode.
Materials and Methods
We conducted a single-centre retrospective study including all neonates born at the Third Department of Obstetrics & Gynecology, School of Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, Greece and admitted to the NICU from January 2022 through December 2024. Data were collected on sex, gestational age, birthweight, mode of delivery, primary cause of admission, feeding route and outcomes including survival and length of hospital stay.
Gestational age was grouped into: <28 weeks (extremely preterm), 28–31 weeks (very preterm), 32–36 weeks (moderate/late preterm), ≥37 weeks (term). Birthweight was categorized as extremely low birthweight (ELBW, <1000 g), very low birthweight (VLBW, 1000–1499 g), low birthweight (LBW, 1500–2499 g) and normal birthweight (≥2500 g). Causes of admission included: prematurity, respiratory problems, respiratory distress syndrome (RDS), jaundice, infections, gastrointestinal disorders, hypoglycemia, other and unknown. In this study, “prematurity” was used as the primary cause of admission when no other acute diagnosis (e.g., respiratory distress, infection) was identified and when the infant required NICU care solely due to immaturity.
Statistical analyses were performed using R and Python. Fisher’s exact and chi-square tests were used for categorical variables. For continuous variables, Mann-Whitney U, one-way ANOVA, or Kruskal-Wallis tests were applied, depending on the distribution. The Cochran-Armitage trend test was used to assess trends in proportions across the three years for LBW and VLBW categories. Significance was set at p<0.05. Survival was calculated per gestational age and birthweight category. Trend analysis across years and post hoc pairwise tests were performed with Bonferroni correction.
Results
A total of 561 neonates were included in the analysis. Male to female ratio was approximately 1:1. The gestational age distribution was: <28 weeks: 4.3%, 28–31 weeks: 8.9%, 32–36 weeks: 38.7%, ≥37 weeks: 48.1%. LBW (<2500g) accounted for 60% of admissions and among them, 17% were VLBW (<1500g).
Figure 1 shows the distribution of LBW and VLBW admissions over the three years of the study. LBW admissions slightly decreased from 62.5% in 2022 (125/200) to 61.2% in 2023 (74/121), and then further to 54.9% in 2024 (123/224). VLBW rates were 18.5% (37/200) in 2022, dropped to 10.7% (13/121) in 2023, and increased again to 18.8% (42/224) in 2024 (Figure 1). Cochran-Armitage trend test showed no statistically significant trend across years (LBW: p = 0.139; VLBW: p = 0.887) ( Figure 1). The fluctuation in VLBW rates across years may reflect changes in referral patterns or local NICU admission thresholds, which were not controlled in this study.
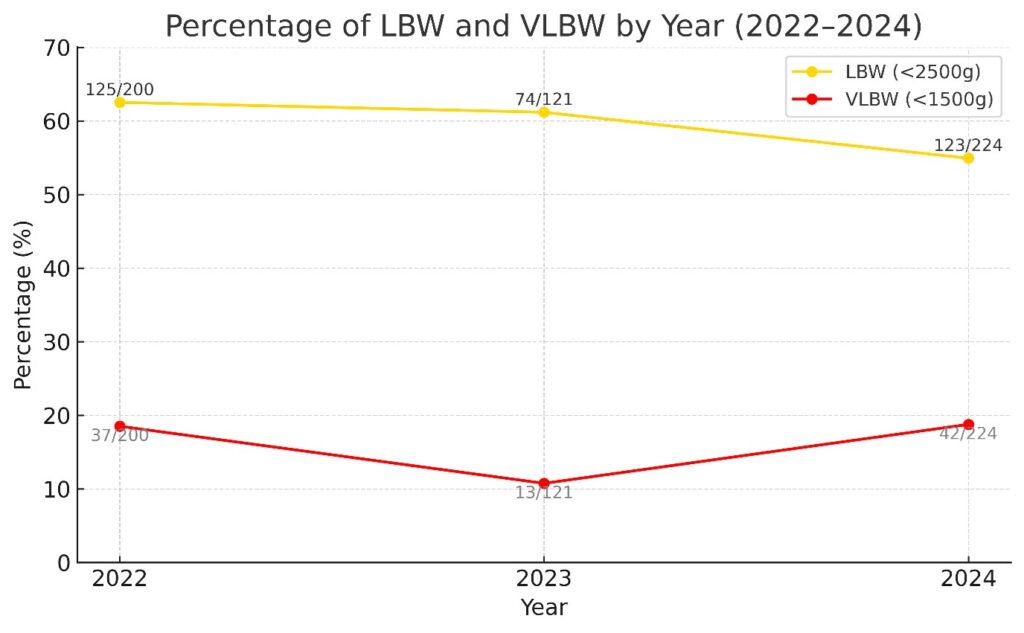
Figure 1: Annual distribution of LBW and VLBW admissions from 2022 to 2024.
Prematurity was the leading cause of admission (48.0%) (Table 1). Respiratory problems (13.1%), other causes (21.9%), and unknown reasons (12.0%) followed. Less common were gastrointestinal issues (1.9%), jaundice (1.1%), RDS (1.1%), hypoglycemia (0.7%), and infections/sepsis (0.4%). Figure 2 displays the cause-specific distribution of admissions in percentage terms.
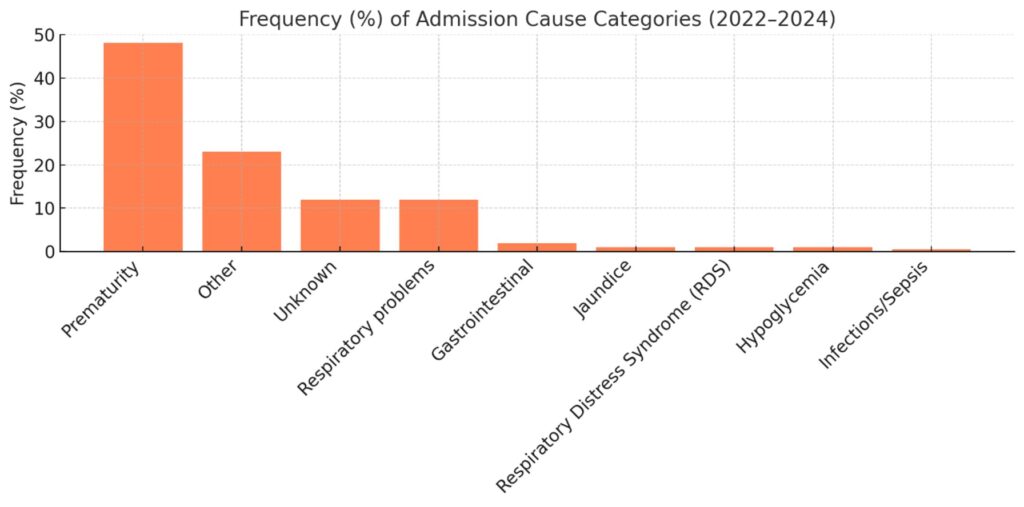
Figure 2: Distribution of causes of NICU admission (2022–2024), showing the proportions of prematurity, respiratory problems, RDS, jaundice, infections, gastrointestinal disorders, hypoglycemia, other, and unknown causes.
Prematurity admissions had significantly lower gestational age and birthweight and longer hospital stays (p<0.001) (Figure 3).
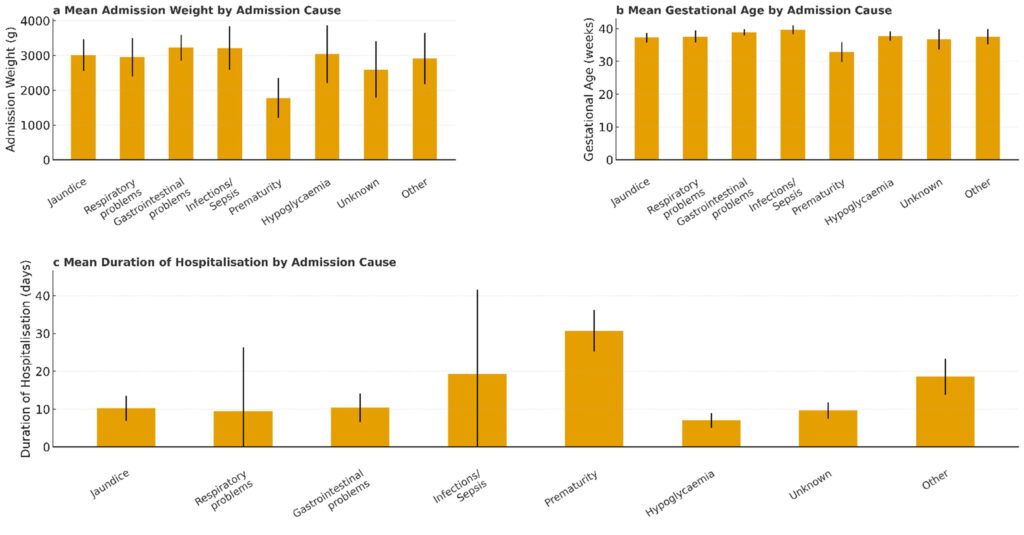
Figure 3: Neonatal outcomes stratified by cause of admission.
(a) Mean birthweight (grams), (b) mean gestational age (weeks), and (c) mean length of hospital stay (days) across different admission causes. Categories include jaundice, respiratory problems, gastrointestinal conditions, infection/sepsis, prematurity, hypoglycaemia, unknown, other. Error bars indicate the standard deviation (SD) in panels a and b, and the 95% Confidence Interval (CI) in panel c.
Respiratory causes showed wide variation in weight and age. Infants with “unknown” or “other” causes were mostly term with short hospitalization. Overall survival to discharge was 97.2%. Survival by gestational age is illustrated in Table 2 and Figure 4.
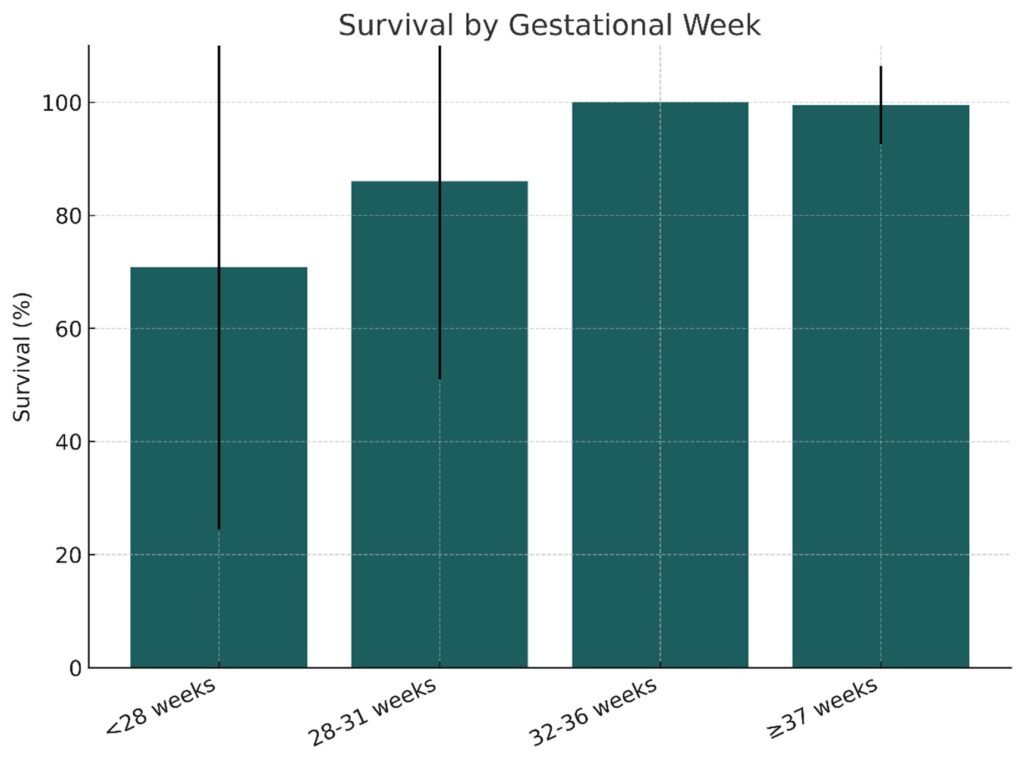
Figure 4: Survival by gestational age group. Error bars represent standard deviation (SD).
Survival improved significantly with increasing GA (p<0.001). Survival by birthweight followed a similar trend (p<0.01) (Table 3, Figure 5).
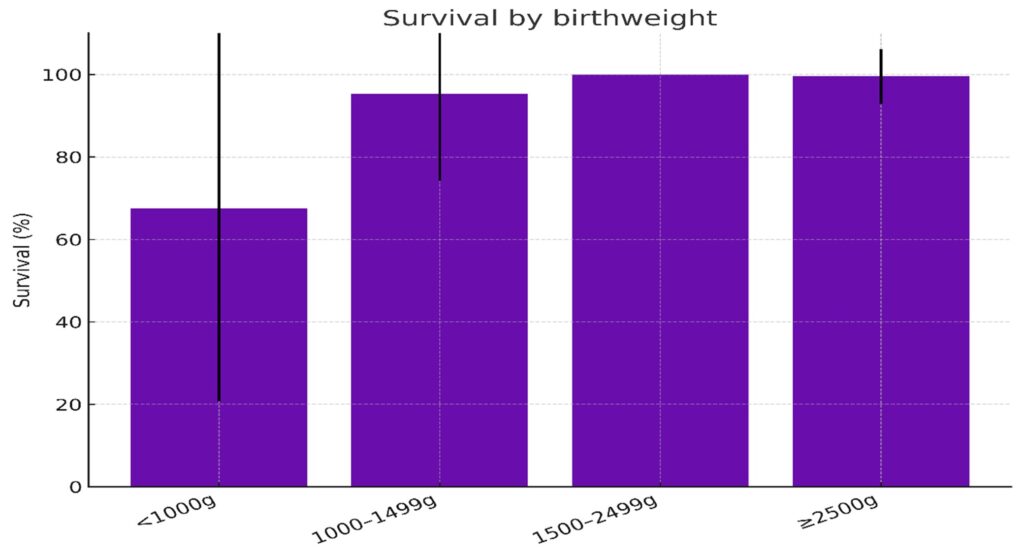
Figure 5: Survival by birthweight category. Error bars represent the standard deviation (SD).
Cesarean section was associated with higher survival in neonates <28 weeks (p=0.006) (Figure 6a), but not in older gestational age groups. No survival difference was found by birthweight (p>0.05) (Figure 6b).
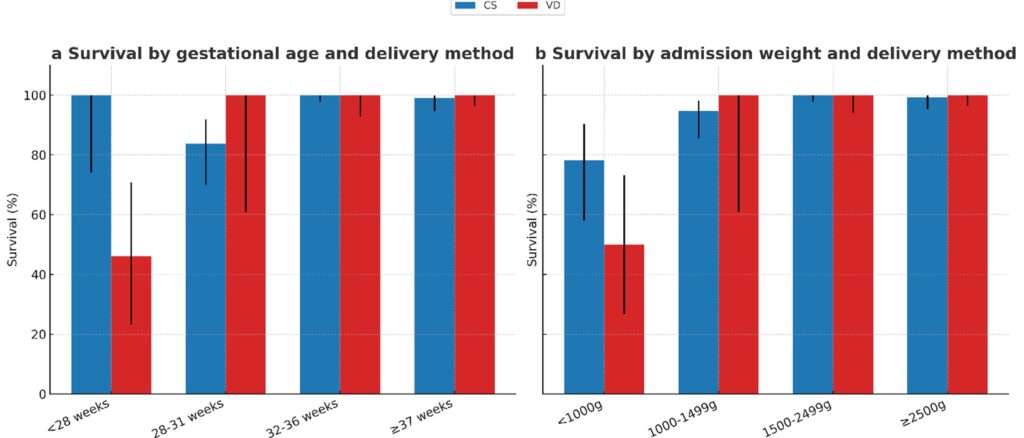
Figure 6: Neonatal survival stratified by mode of delivery across gestational age and birthweight categories.
(a) Survival (%) by gestational age group and delivery type (CS: Cesarean section, VD: Vaginal delivery).
(b) Survival (%) by admission weight group and delivery type. Error bars represent the 95% CI.
Feeding method at discharge (bottle vs tube) did not significantly affect hospital stay (p=0.89) (Figure 7).
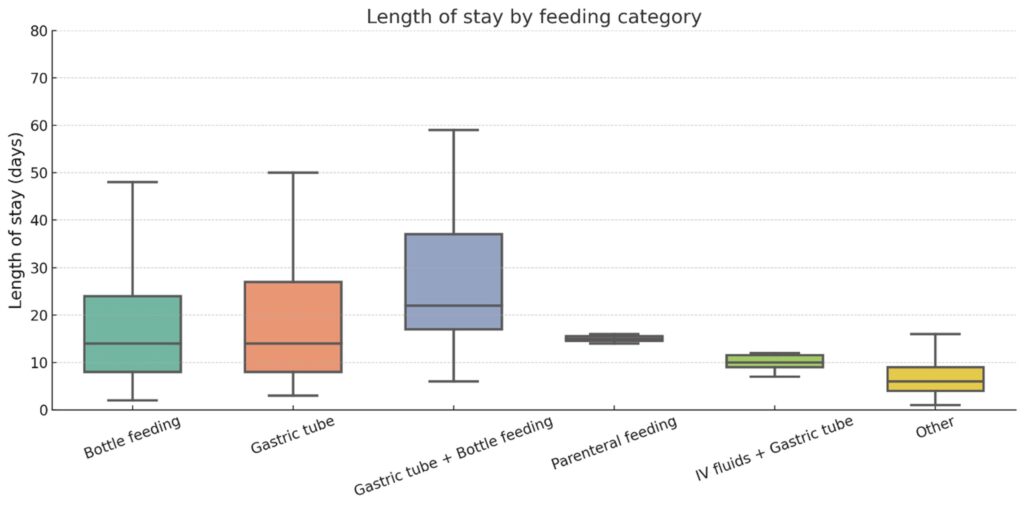
Figure 7: Length of hospital stay by feeding category.
Boxplot showing the duration of hospitalization (days) across different feeding methods, including bottle feeding, gastric tube, parenteral feeding, and intravenous fluids. Central lines indicate medians; whiskers represent the range. Error bars represent standard deviation.
Discussion
We found that: 1) prematurity remains the dominant cause of NICU admissions and the most critical factor influencing survival and morbidity, 2) gestational age and birthweight were the most important predictors of survival and 3) cesarean delivery may confer benefits at the extreme prematurity, while feeding route at discharge does not appear to impact hospitalization duration.
Our findings align with global findings reported by the WHO and other large-scale neonatal cohorts (1,2). The 48% admission rate for prematurity observed in our cohort mirrors similar statistics in international NICU surveillance studies, underlining the global burden of preterm birth (1).
The associations between low gestational age, low birthweight, and increased hospitalization duration are well established in neonatal research (3,6). Our results reflect these associations clearly, as demonstrated by significantly lower birthweight and gestational age in infants admitted for prematurity, and longer stays compared to other causes. This trend has been supported by previous work from UK and European datasets showing that birthweight and maturity are powerful predictors of NICU outcomes (5,6)
The stepwise improvement in survival with increasing gestational age and birthweight is in line with other recent neonatal studies, including national reports from high-income countries that show substantial gains in survival after each completed gestational week (5,11). Similar findings were reported in a study, where perinatal outcomes improved markedly between 22 and 28 weeks of gestation (12).
Our observation that cesarean section improved survival in neonates <28 weeks is consistent with results from cohort studies suggesting delivery mode can influence outcomes at the limit of viability (13,14). This is further supported by a meta-analysis, which suggested cesarean delivery is associated with improved survival among extremely preterm infants (15). However, individualized delivery planning based on fetal condition and institutional viability policies remains essential.
Although feeding method at discharge did not significantly impact length of stay in our sample, numerous studies emphasize the benefits of early enteral nutrition and human milk feeding for preterm infants; these benefits include improved gastrointestinal tolerance and better neurodevelopmental outcomes, especially in VLBW neonates (16–18). Differences in timing of initiation and feeding advancement may explain this discrepancy in our cohort.
This study has certain limitations; its retrospective nature should be considered as the major one; however, there were no missing data, because of the digital recording of all deliveries. Moreover, the single-center design, as well as the relatively small sample size may not allow the generalizability of the findings.
Conclusions
This study highlights prematurity as the leading driver of NICU admissions and adverse outcomes, with gestational age and birthweight as the strongest survival predictors. Cesarean delivery appears beneficial at the threshold of viability, while feeding route at discharge has limited impact. These findings emphasize the urgent need for targeted perinatal strategies to improve survival and reduce morbidity among extremely preterm and very low birthweight infants.
Conflict of Interest
None.
Source of Funding
None.
References
- Liang X, Lyu Y, Li J, Li Y, Chi C. Global, regional, and national burden of preterm birth, 1990–2021: a systematic analysis from the global burden of disease study 2021. eClinicalMedicine. 2024 Oct 1;76. Available from: https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(24)00419-X/fulltext
- World Health Organization. Born too soon: decade of action on preterm birth. Geneva; 2023. Available from: https://www.who.int/publications/i/item/9789240073890
- AlQurashi MA. Impact of Mode of Delivery on the Survival Rate of Very Low Birth Weight Infants: A Single-Center Experience. Cureus. 2020 05;12(12):e11918.
- Mukerji A, Shah PS, Kadam M, Borhan S, Razak A. Non-invasive respiratory support in preterm infants as primary mode: a network meta-analysis. Cochrane Neonatal Group, editor. Cochrane Database Syst Rev. 2025 July 17;2025(7):Art. No.: CD014895.
- Glass HC, Costarino AT, Stayer SA, Brett CM, Cladis F, Davis PJ. Outcomes for Extremely Premature Infants. Anesth Analg. 2015 June;120(6):1337.
- Seaton SE, Agarwal R, Draper ES, Fenton AC, Kurinczuk JJ, Manktelow BN, et al. Estimated neonatal survival of very preterm births across the care pathway: a UK cohort 2016–2020. Arch Dis Child – Fetal Neonatal Ed. 2023 Nov 1;108(6):562–8.
- Malloy MH, Doshi S. Cesarean Section and the Outcome of Very Preterm and Very Low-Birthweight Infants. Clin Perinatol. 2008 June 1;35(2):421–35.
- Jarde A, Feng YY, Viaje KA, Shah PS, McDonald SD. Vaginal birth vs caesarean section for extremely preterm vertex infants: a systematic review and meta-analyses. Arch Gynecol Obstet. 2019 Dec 24;301(2):447–58.
- Kumar RK, Singhal A, Vaidya U, Banerjee S, Anwar F, Rao S. Optimizing Nutrition in Preterm Low Birth Weight Infants—Consensus Summary. Front Nutr . 2017 May 26; 4. Available from: https://www.frontiersin.org/journals/nutrition/articles/10.3389/fnut.2017.00020/full
- Chitale R, Ferguson K, Talej M, Yang WC, He S, Edmond KM, et al. Early Enteral Feeding for Preterm or Low Birth Weight Infants: a Systematic Review and Meta-analysis. Pediatrics. 2022 Aug 1;150(Supplement 1):e2022057092E.
- Rodriguez-Sibaja MJ, Herrera-Ortega O, Lumbreras-Marquez MI, Morales-Barquet D, Acevedo-Gallegos S, Copado-Mendoza Y, et al. Survival assessment in extremely preterm neonates in a middle-income setting. Front Pediatr. 2025 May 30; 13. Available from: https://www.frontiersin.org/journals/pediatrics/articles/10.3389/fped.2025.1574613/full
- Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, et al. Neonatal Outcomes of Extremely Preterm Infants From the NICHD Neonatal Research Network. Pediatrics. 2010 Sept 1;126(3):443–56.
- Czarny HN, Forde B, DeFranco EA, Hall ES, Rossi RM. Association between mode of delivery and infant survival at 22 and 23 weeks of gestation. Am J Obstet Gynecol MFM. 2021 July 1;3(4):100340.
- Higgins BV, Baer RJ, Steurer MA, Karvonen KL, Oltman SP, Jelliffe-Pawlowski LL, et al. Resuscitation, survival and morbidity of extremely preterm infants in California 2011–2019. J Perinatol. 2024 Feb;44(2):209–16.
- Unger V, Gasparics Á, Nagy Z, Hernádfői M, Nagy R, Walter A, et al. Cesarean delivery is associated with lower neonatal mortality among breech pregnancies: a systematic review and meta-analysis of preterm deliveries ≤32 weeks of gestation. Am J Obstet Gynecol. 2024 Dec 1;231(6):589-598.e21.
- Ford SL, Lohmann P, Preidis GA, Gordon PS, O’Donnell A, Hagan J, et al. Improved feeding tolerance and growth are linked to increased gut microbial community diversity in very-low-birth-weight infants fed mother’s own milk compared with donor breast milk. Am J Clin Nutr. 2019 Apr 1;109(4):1088–97.
- Hair AB, Patel AL, Kiechl-Kohlendorfer U, Kim JH, Schanler RJ, Hawthorne KM, et al. Neurodevelopmental outcomes of extremely preterm infants fed an exclusive human milk-based diet versus a mixed human milk + bovine milk-based diet: a multi-center study. J Perinatol. 2022 Nov;42(11):1485–8.
- Quitadamo PA, Comegna L, Zambianco A, Palumbo G, Gentile MA, Mondelli A. Impact of Enteral Nutrition on Clinical Outcomes in Very Low Birth Weight Infants in the NICU: A Single-Center Retrospective Cohort Study. Nutrients. 2025 Jan;17(7):1138.