Research
HJOG 2026, 25 (2), 102-120| doi: 10.33574/hjog.0621
Nsreen Zakarya Hassan1, Sabah Lofty Mohamed2, Amina Saad Gonied2
1Al Ahrar Hospital, Zagazig, Egypt
2Zagazig University, Zagazig, Egypt
Correspondence: Nsreen Zakarya Hassan, E-mail: Nsreenzakarya42@gmail.com
![]()
Abstract
Background: Effective postpartum pain management is crucial for maternal well-being and recovery. Nurses play a pivotal role in assessing and managing postpartum pain, yet many face knowledge deficits and systemic barriers that hinder optimal care delivery. Structured education may bridge this gap and enhance pain management practices.
Objective: To assess the effect of a structured educational program on nurses’ attitudes and perceived barriers regarding pain relief measures for postpartum mothers at Al-Ahrar Hospital.
Methods: A quasi-experimental one-group pretest-posttest design was used. The study included all nurses (n = 20) working in the postpartum ward of Al-Ahrar Hospital, Zagazig City, Egypt. Data collection tools included a structured questionnaire measuring nurses’ attitudes toward postpartum pain assessment and management and the barriers they encounter. A structured educational program focusing on both pharmacological and non-pharmacological pain relief was implemented over multiple sessions.
Results: There was a statistically significant improvement in nurses’ attitudes toward postpartum pain relief post-intervention (p < 0.001). Before the program, 80% of nurses exhibited negative attitudes; after the intervention, 100% demonstrated positive attitudes. Similarly, reported barriers—mother-related, nurse-related, physician-related, and systemic—were significantly reduced post-intervention. Strong positive correlations were found between the educational program and improved attitudes (r = 0.906) and barrier reduction (r = 0.898), with a high correlation between attitude and barrier scores (r = 0.962).
Conclusions: The structured educational program was effective in enhancing nurses’ attitudes and reducing perceived barriers to postpartum pain relief. These findings support the integration of regular educational interventions into clinical practice to improve the quality of postpartum care.
Keywords: Postpartum pain, nurses’ attitudes, pain management, educational program, non‐ pharmacological methods, barriers to care
Introduction
The postpartum period is indeed a critical phase for women, as they need to balance their own recovery with the demands of caring for their newborns. Many women tend to prioritize the needs of their infants over their own, which can impact their health and well-being in both the short term and long term. It is essential for mothers to also focus on self-care during this time to ensure they can adequately support their infants (1).
The trend toward hospital opioid use is widespread, and the postpartum period is no different. Opioids are commonly used in this period in hospitals and are prescribed upon discharge (2). Non-pharmacological pain relief methods can be used to relieve pain, alleviate suffering, and promote women‟s health during labor (3). It is safe for both mother and fetus, does not cause side effects, and postpones the use of pharmacological pain relievers. also, it reduces the negative outcomes associated with pharmacological pain relief methods and improves obstetric outcomes (4).
Nurses recognized the importance of individualized pain management and opioid use in patients but sought enhancements in training and the creation of evidence-based protocols. They play a crucial role in postpartum pain relief by recommending various measures. Commonly suggested methods include the use of ibuprofen and acetaminophen for pain management, as well as non-pharmacological approaches like applying ice packs to the perineal area for 10 to 20 minutes, especially within the first 24 to 72 hours after childbirth. Additionally, nurses may encourage techniques such as changing positions and practicing deep breathing exercises to help manage discomfort (5).
According to ACOG, at least 40% of women do not seek postpartum care. Several factors contribute to this trend, such as cultural differences, lack of insurance, lack of adequate family support, low socioeconomic status, poor anticipatory guidance, race, lack of good transitional care management, and poor access to home visits. According to the Pregnancy Mortality Surveillance System, non-Hispanic blacks have the highest maternal mortality (6).
The knowledge and attitudes of obstetric care providers (OCPs) towards non- pharmacological pain relief methods (NPPR) during the postpartum period significantly impact their utilization of these methods. Research indicates that about 66.9% of OCPs lack adequate knowledge and 65.5% hold unfavorable attitudes towards NPPR, which contributes to a 30.4% underutilization rate. Barriers to implementing NPPR include systemic barriers, practitioner barriers, and patient factors, highlighting a need for improved education and support for OCPs to enhance the adoption of these methods (7, 8).
There is a notable gap between obstetric care providers’ knowledge and attitudes regarding non-pharmacological pain relief and its practical application. Barriers such as patient beliefs, time constraints, and workload significantly hinder the implementation of these methods. Cultural differences, healthcare policies, and specific clinical settings further influence attitudes and practices related to non- pharmacological pain management. Addressing these barriers is essential for improving the utilization of effective pain relief strategies during postpartum (9).
The aim of our study was to evaluate the effectiveness of a structured educational program in improving nurses’ attitudes and reducing perceived barriers toward the use of pain relief measures for postpartum mothers. Recognizing that postpartum pain management is often undervalued in clinical practice—especially in resource-limited settings—the study sought to empower nurses with the knowledge and skills necessary to assess and manage pain effectively. By focusing on both pharmacological and non-pharmacological interventions, the educational program aimed to foster a more patient-centered approach to care, enhance nurses’ confidence, and address institutional and professional challenges that hinder optimal pain relief.
Subjects and Method
This study employed a quasi-experimental one-group pretest-posttest design to evaluate the effectiveness of a structured educational program. The study was conducted at the postpartum inpatient ward of Al-Ahrar Hospital, a governmental tertiary care facility located in Zagazig City, Egypt. The research took place from June 2024 to July 2025, allowing sufficient time to implement the intervention and collect both pre- and post-intervention data.
Study Population and Sample Size
The study population included all registered nurses working in the postpartum ward at the time of the study. A convenience sampling technique was used, and a total of 20 nurses were recruited. This complete enumeration of the available target group ensured maximal participation within the study setting.
Inclusion and Exclusion Criteria
Inclusion Criteria:
- All female nurses working in the postpartum unit.
- Nurses who provided verbal consent to participate.
- Nurses available during the educational intervention period.
Exclusion Criteria:
- Nurses on extended leave or rotated to other departments during the study period.
- Nurses who refused to participate or withdrew at any time.
Tools of data collection
The researchers developed data collection tools based on similar studies, prepared in English, and included three parts:
Part (A): Demographic Characteristics of Nurses. This included age, gender, residency, and educational level. It also covered years of experience, marital status, attendance at educational programs related to postpartum pain management, as well as the number and duration of training courses on postpartum pain relief measures.
Part (B): Nurses’ Attitudes towards Pain Relief Measures during the Postpartum Period. This included:
- Nurses’ Attitudes Toward Postpartum Pain Assessment. This section included six items aimed at understanding nurses’ perceptions regarding postpartum pain assessment, such as: 1. A mother may shout for many reasons, not just because of postpartum pain. 2. Pain should be assessed before and after using postpartum pain relief measures. 3. Every mother experiences postpartum pain differently. 4. The mother should be advised to use pain relief along with postpartum pain relief measures. 5. Understanding postpartum pain can help manage it better. 6. Vital signs are always reliable indicators of the severity of postpartum pain.
- Nurses’ Attitudes Toward Postpartum Pain Management. This consisted of nine items that reflect attitudes towards managing postpartum pain, such as: 1. Pain relief is an essential part of postpartum care for mothers. 2. Postpartum pain relief measures are recommended for managing postpartum pain. 3. Pain severity can be determined without asking mothers. 4. Proper assessment of pain is a priority for effective postpartum pain management. 5. Providing comfort and proper positioning for the mother can help reduce muscle strain, which may alleviate postpartum pain. 6. Combining non-pharmacological and pharmacological approaches is practical for pain management and has fewer side effects. 7. Nurses have a responsibility and obligation to manage pain. 8. The nurse is the best person to determine what the mother is feeling in pain. 9. Non-pharmacological interventions (such as music, imagination, and touch) are effective for controlling mild to moderate pain but are rarely helpful in severe cases.
- Attitudes of Nurses Regarding the Effect of Pain-Relief Methods during Postpartum. This section consisted of seven items relating to nurses’ beliefs about the effectiveness of pain relief measures: 1. Women should expect pain during the postpartum period. 2. It is believed that postpartum pain relief is necessary. 3. The use of postpartum pain relief measures will affect the progress of the postpartum period. 4. Postpartum pain relief measures are considered safer during this time. 5. Such measures will enhance maternal comfort. 6. Opinions about the effect of postpartum pain relief measures on a mother’s ability to cope with pain. 7. Concerns about the use of postpartum pain relief measures during the postpartum period.
Scoring System
Nurses’ attitudes toward postpartum pain relief measures are assessed using a 2-point Likert scale, with responses categorized as agree (1) or disagree (0). Participants are classified as having a positive or negative attitude based on their scores.
Part (C): Barriers to the Use of Postpartum Pain-Relief Methods. It Developed by the researchers based on a literature review, this identified 23 barriers to using postpartum pain relief methods.
- Mother-Related Barriers. Barriers faced by the mother include: inability to communicate, hemodynamic instability, and history of drug abuse or suicide attempts, which can impede effective pain management.
- Nurse-Related Barriers. This included five barriers: poor understanding and interpretation of pain behaviors, insufficient knowledge of pain relief interventions, lack of education and training in pain assessment, management, and emotional care as well as failure to consider physiological indicators, and conditions that enhance pain perception.
- Physician-Related Barriers. Reported barriers included: Poor interaction between physicians and nurses regarding nonverbal cues indicating maternal pain, lack of experience and heavy workloads among physicians.
- Healthcare System Barriers. This included 14 barriers such as: Absence of standardized pain assessment tools for both verbal and nonverbal critically ill mothers, lack of standardized guidelines and protocols for pain assessment and management, heavy nurse workloads and staff shortages, inadequate nurse-to- mother ratios and training on pain management. As well as complicated discussions regarding pain management that are ineffective, poor documentation of pain assessment results, lack of independent decision-making regarding pain management, and unsatisfactory hospital environments, such as shared rooms with minimal privacy.
Scoring System
A modified Likert scale assesses perceived barriers, with responses categorized as having barriers if they agree (1) or not having barriers if they disagree (0).
Part (D): Nurses’ Education Program Regarding Postpartum Pain Relief Measures. The goal of this education program was to ensure that nurses are well- equipped with the knowledge and resources necessary to effectively support mothers during the postpartum period. By enhancing nurses’ skills in managing and alleviating postpartum pain, improve maternal comfort and overall care. This initiative concentrated on the education and training provided by researchers regarding various postpartum pain relief measures, emphasizing the need for nurses to be informed and competent in their approach to pain management for new mothers. Through this targeted education, the program seeks to foster a more supportive and effective healthcare environment for postpartum patients.
Components of Nursing Education on Postpartum Pain Relief
The program emphasized the importance of educating nurses about various postpartum pain relief measures. It covered both pharmacological and non- pharmacological approaches, enabling nurses to provide comprehensive care to mothers experiencing pain after childbirth.
Supportive Material: The researchers had compiled a literature review that had been transformed into a user-friendly booklet (brochure). This brochure included descriptive content designed to bolster nurses’ understanding and awareness of postpartum pain relief methods. The material highlights: Different types of pain relief options available to mothers. – Best practices for pain assessment and management, as well as techniques for effective communication with mothers regarding their pain experiences and evidence-based guidelines for administering pain relief interventions.
Validity of Tools: The data collection tools were assessed for validity by a panel of three experts of professors specializing in obstetrics and gynecological nursing. These experts evaluated the tools for clarity, relevance, and the time required for completion. Based on their feedback, necessary modifications were made to enhance the tools’ effectiveness and appropriateness for the study.
Reliability of Tools: To establish the reliability of the tools, internal consistency was tested using Cronbach’s alpha. The results included: Attitude Tool: [0.906] and Barrier Tool: [0.926]. These values indicate the stability and internal consistency of the tools utilized in the study, ensuring that they effectively measure what they are intended to assess.
Pilot Study: A pilot study was conducted on a sample representing 10% of the overall study sample, specifically involving 2 nurses selected from the previously mentioned study setting. The findings from the pilot study were analyzed, leading to necessary adjustments to the tools and methodology. The subjects included in the pilot study were incorporated into the main study sample, ensuring comprehensive data collection and analysis.
Procedure: The study was conducted in three distinct phases:
- Assessment Phase (Pre-Test): During the initial phase, the researchers began with an introductory meeting with the nurses in the postnatal unit. In this meeting, the researcher introduced herself and explained the study’s objectives, nature, duration, and the various activities involved. This phase was crucial for establishing rapport and ensuring that the nurses understood the importance of their participation in the study.
- Implementation Phase (Conducting Health Educational Program): After securing the nurses’ consent to participate in the study, the researcher provided an overview of the educational program. She clarified the questions in the assessment tool, ensuring that the nurses comprehended the content and purpose of the program. This phase involved delivering the health education focused on postpartum pain relief measures, aimed at enhancing the nurses’ attitudes and their barriers. The researcher ensured an educational environment that was convenient for participants and organized the sessions to fit within the available time. This occurred twice a week from 10:00 to 12:00 AM, with session averaging 20-25 minutes. Each session began with a summary of prior content to reinforce understanding among the nurses.
The researcher utilized simple language appropriate for all educational levels and incorporated motivational techniques, such as praise and recognition, to foster an engaging learning atmosphere. Maintaining control and regulating discussion along the session guidelines was fundamental in facilitating effective learning experiences. An average of 10 to 12 educational sessions was conducted throughout the data collection period. At the conclusion of the educational sessions, the researcher provided a summary of the program’s objectives while acknowledging each nurse’s participation
- Evaluation Phase (Post-Test): In the final phase, following the educational program, the researcher interviewed each nurse individually again, administering the questionnaire as before to assess their attitudes and barriers regarding postpartum pain and relief measures. The evaluation of the program occurred twice, immediately after the program’s implementation. The pre-test and post-test results allowed for a comparison of nurses’ attitudes and their barriers through the educational program.
Statistical Design: The collected data were organized and analyzed using the appropriate statistical significance tests. It collected and coded using the Computer Statistical Package for Social Science (SPSS), version 25. The data were presented using descriptive statistics in the form of frequencies and percentages. Graphs were done for data visualization using Microsoft Excel. For qualitative (categorical) variables categorical variables were compared using the chi-square test. Paired Samples t tests were used to compare mean scores. The degrees of significance of the results were considered as follows: P-value > 0.05 Not significant P-value ≤ 0.05 – ≤ 0.01 Highly Significant.
Results
Table (1) shows that 55.0% of nurses aged between 31-40 years. Concerning gender and residence, 100% and 75.0% were females and urban residents. Regarding the level of qualification and years of experience, 50.0% and 35.0% of them had a technical institute for nursing and more than 10 years, respectively. Furthermore, 80.0% and 55.0% of them were married and had not attended any educational programs on postpartum pain. The same table revealed that 27.5% of them had not received training courses on postpartum pain.
Table (2) shows that 65.0% and 60.0% of nurses disagreed that mothers should be advised to use analgesics with pain relief measures and that vital signs are always reliable indicators of postpartum pain severity, respectively. After the intervention, 100.0%, 100.0%, and 100.0% of them agreed that during the postpartum period, the mother may cry for many reasons other than postpartum pain, and pain should be assessed before and after pain relief measures, as well as understanding postpartum pain may help better management. There was a statistically significant difference in nurses’ attitudes toward the assessment of postpartum pain before and after the intervention (p < 0.05).
Table (3) shows that 65.0%, 65.0%, 70.0%, and 65.0% of the nurses disagreed with the idea that pain relief is an essential part of postpartum care, pain relief measures for postpartum pain is not recommended, appropriate pain assessment is not a priority for effective postpartum pain management and combining non- pharmacological and pharmacological methods is not practical for pain management or fewer side effects, respectively. After the intervention, 100.0%, 100.0%, and 100.0% of them agreed that pain relief is an essential part of maternal postpartum care, appropriate pain assessment is a priority for effective postpartum pain management, and providing comfort and proper positioning for the mother can help reduce muscle strain which may reduce postpartum pain. There was a statistically significant difference in nurses‟ attitudes towards postpartum pain management before and after the intervention (p < 0.05).
Table (4) shows that 70.0%, 70.0%, 80.0%, and 70.0% of the nurses disagreed that mothers should expect pain during the postpartum period, the use of methods will affect the progress of the postpartum period, opinions on the effect of pain relief measures on the mother’s ability to cope with pain, and concerns about the use of pain relief measures during the postpartum period, respectively. After the intervention, 100.0%, 100.0%, and 100.0% of them agreed that mothers should expect pain during the postpartum period, believed that pain relief during the postpartum period is necessary, opinions on the effect of pain relief measures on the mother’s ability to cope with pain, and concerns about the use of pain relief measures during the postpartum period. There was a statistically significant difference between the nurses on the effect of pain relief measures during the postpartum period before and after the intervention (p < 0.05).
Table (5) & figure (1) shows that 55.0%, 80.0%, 85.0%, and 80.0% of nurses had negative attitudes regarding postpartum pain assessment, postpartum pain relief management, the effect of pain-relief methods during postpartum and total attitude levels before the intervention compared to after the intervention, about 100.0% of them had positive attitudes, respectively. There was a statistically significant difference in attitudes between before and after the intervention (P < 0.000).
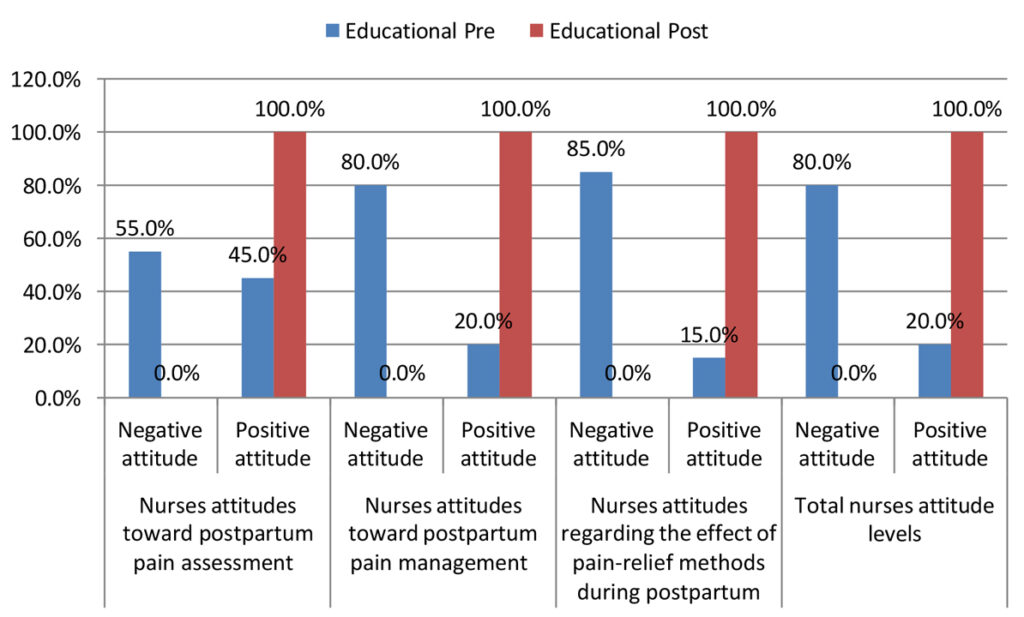
Figure 1. Levels of nurses’ attitude about postpartum pain (no=20).
Concerning the barriers faced by mothers in using postpartum pain relief methods, table (6) shows that 60.0% and 65.0% of nurses before the intervention did not agree with mothers‟ preferences/beliefs and their inability to communicate compared to 10.0% and 10.0% after the intervention, respectively. There was a statistically significant difference between before and after the intervention (P < 0.05).
Concerning the barriers faced by nurses regarding using postpartum pain relief methods, table (7) shows that 60.0% and 65.0% of nurses disagreed with the lack of education, and training regarding pain assessment, management and emotional care, and failure to consider physiological indicators, respectively, were barriers related to the use of postpartum pain relief methods pre-intervention. After the intervention, 100.0%, 100.0%, and 100.0% of them agreed that poor understanding and interpretation of pain behaviors, lack of education and training regarding pain assessment, management / emotional care, failure to consider physiological indicators, and failure to improve mothers‟ perception of pain were barriers related to the use of postpartum pain relief methods. There was a statistically significant difference between pre-and post- intervention (p < 0.05).
Table (8) shows that before the intervention, only 35.0% of nurses did not agree that poor interaction between physicians and nurses regarding a mother’s non- verbal pain hinders effective treatment as an obstacle for physicians to use postpartum pain relief methods. After the intervention, 100.0% and 100.0% of them agreed that poor interaction between physicians and nurses regarding maternal non-verbal pain also hinders effective treatment, and lack of experience and heavy workloads of physicians were obstacles for physicians to use postpartum pain relief methods. There was a statistically significant difference between before and after the intervention (p < 0.05).
Table (9) shows that before the intervention, 70.0% & 70.0% of nurses agreed that heavy nurse workload and shortage of nursing staff were obstacles for the health system to use postpartum pain relief methods. After the intervention, 100.0%, 100.0% & 100.0% of them agreed that heavy nurse workload, shortage of nursing staff, and non-therapeutic, ineffective, or complicated discussions about pain management during medical rounds were obstacles for the health system to use postpartum pain relief methods. There was a statistically significant difference between before and after the intervention (p < 0.05).
Table (10) shows that 80.0% of nurses reported that physicians were a barrier to the use of postpartum pain relief before the intervention compared to 100.0% of them reported that barriers related to mothers, nurses, physicians, and the health system were an obstacle to the use of postpartum pain relief after the intervention. There was a statistically significant difference in attitudes between before and after the intervention (P < 0.000).
Table (11) shows that there is a strong positive correlation (0.906 and 0.898) between the program and nurses‟ attitudes and barriers regarding postpartum pain- relief methods. It was also found that there is a strong positive correlation (0.962) between nurses‟ attitudes and barriers. It was also noted that there were highly statistically significant differences regarding postpartum pain-relief methods (P < 0.000).
Discussion
Pain management during the postpartum period remains a critically under-addressed area in maternal healthcare, particularly in resource-limited settings. Despite the availability of both pharmacological and non-pharmacological pain relief methods, a significant proportion of postpartum women continue to experience unmanaged or poorly managed pain. This often stems not from a lack of treatment modalities, but rather from barriers faced by frontline caregivers—especially nurses—who are pivotal in the provision of postpartum care. These barriers may include insufficient knowledge, inadequate training, limited institutional support, and attitudinal biases. Although several international guidelines advocate for comprehensive pain management, real-world practice often lags, especially in developing healthcare systems (8, 10). Thus, there is a distinct gap in the literature and clinical practice regarding the education and empowerment of nurses in this critical domain.
The rationale for this study was grounded in the observed inconsistency between available evidence-based pain relief strategies and the limited implementation of these practices in hospital postpartum wards. Nurses’ attitudes and perceived barriers significantly influence how pain is assessed and managed. Without structured education, nurses may undervalue non-pharmacological interventions, rely on subjective cues such as vital signs, and underutilize evidence-based methods. Recognizing this discrepancy provided the impetus to design an intervention that could shift these attitudes and reduce institutional and personal barriers to pain relief (11).
The novelty of this study lies in its comprehensive approach to tackling both cognitive (knowledge and attitudes) and structural (barriers) aspects of postpartum pain management within a real clinical setting. Unlike previous research that often isolates theoretical knowledge from clinical practice, this study bridges that gap by implementing a targeted educational program and directly measuring its impact through pre- and post-intervention assessments (11, 12).
Conducted in the postpartum ward of Al-Ahrar Hospital, Zagazig City, Egypt, the study was situated in a setting representative of many public hospitals in low- and middle-income countries, where staff shortages, high patient loads, and systemic inefficiencies frequently obstruct optimal maternal care. The hospital provided a practical environment to assess how a structured, scalable educational intervention could influence care delivery without the need for costly resources or extensive infrastructure changes.
The aim of this study was to determine the effect of a structured educational program on nurses’ attitudes and the barriers they face in applying postpartum pain relief measures. By identifying and addressing both the perceptual and institutional obstacles, the study seeks to improve the quality of postpartum pain management and set a precedent for scalable, evidence-based nursing education programs. In essence, we performed this study to demonstrate that empowering nurses through focused education can lead to meaningful improvements in clinical care, especially in settings where maternal pain is often overlooked or minimized.
Regarding Improvement in Nurses’ Attitudes Toward Postpartum Pain Relief, our study revealed a statistically significant improvement in nurses’ attitudes toward postpartum pain relief after implementation of the educational intervention, particularly regarding the necessity of prioritizing pain relief as a core nursing duty. This aligns with Innab et al. (13), where nurses’ mean attitude scores toward pain management significantly improved post-intervention (from M = 20.3 to M = 22.2, p < .01), highlighting that structured pain education effectively alters professional perspectives on pain relief responsibilities.
Ibrahim et al. (14) also documented a similar trend, emphasizing the role of scenario-based training in transforming attitudes toward maternal care, especially around under-addressed postpartum pain needs. This convergence supports the rationale that targeted education fosters empathy and professional responsibility toward maternal pain management.
Regarding Reduction in Perceived Barriers to Pain Relief Implementation, in our study, the perceived barriers, such as lack of time, insufficient protocols, and fear of drug dependency, decreased significantly post-intervention. Nurses reported improved confidence and clarity in implementing analgesic protocols and communicating with patients.
Ramasamy et al. (15) similarly noted that education reduced institutional and personal barriers among nurses in India, especially those related to misconceptions about opioid use and underreporting of pain by patients. In Gaber Zagloul et al. (16), post-intervention responses showed marked reduction in clinical hesitations and increased self-assurance in following evidence-based postpartum care procedures, including pain relief.
Regarding Correlation Between Attitudes and Barriers, our study found a moderate inverse correlation (r = –0.42) between improved attitudes and perceived barriers post-intervention. This suggests that the more favorable the attitude, the fewer obstacles nurses perceived in delivering adequate pain relief.
This finding is echoed in Innab et al. (13), where increased confidence and satisfaction with learning were positively correlated with post-test improvements in knowledge and attitude and reduced hesitation in applying pain protocols. Ibrahim et al. (14) also highlighted a significant reduction in perceived barriers among nurses with positive attitude changes following training, indicating a reinforcing loop between attitude and clinical behavior.
Regarding Demographic Influences on Attitude and Barrier Changes, in our study, younger nurses and those with fewer years of experience exhibited greater improvement in attitudes and perceived fewer barriers after training. This is consistent with Innab et al. (13), where diploma nurses initially lagged behind BSN nurses in baseline scores, but after the intervention, the difference vanished, implying that educational input neutralized disparities across experience and qualification levels.
Gaber Zagloul et al. (16) also reported that less experienced nursing students showed greater gains post-training in both knowledge and attitude, likely due to a more flexible mindset and fewer entrenched clinical habits. Ramasamy et al. (15) supported this by noting significant improvement in novice nurses’ pain relief practices compared to their more experienced peers.
Regarding Overall Effectiveness of the Educational Intervention, our study demonstrated a clear, measurable improvement in knowledge, attitudes, and practical readiness of nurses regarding postpartum pain management following the intervention. The shift was sustained and covered multiple domains—attitude, knowledge, and application—showing the educational model’s robustness.
Similar conclusions were drawn in Gaber Zagloul et al. (16), where the educational guideline improved both theoretical knowledge and skill-based practice regarding postnatal care. Innab et al. (13) also validated the lasting effect of their structured program on pain knowledge and confidence.
Even though Ramasamy et al. (15) had a more limited scope in terms of postpartum specificity, their broader maternal care training intervention significantly improved nurses’ behavior toward respectful and effective post-delivery care, indirectly reinforcing the effectiveness of continued education.
Clinical Implications
The clinical implications of this study are profound, particularly for postpartum maternal care. The results demonstrated that a structured educational program can significantly improve nurses’ attitudes toward pain relief and simultaneously reduce the perceived barriers to implementing effective postpartum pain management. Clinically, this implies that with proper educational support, nurses can transition from relying on limited or outdated pain assessment methods—such as vital signs alone—to embracing holistic, patient-centered approaches. The shift in attitude fosters more empathetic and effective communication with postpartum mothers, allowing for better identification of pain levels and personalized interventions. This not only enhances maternal comfort and satisfaction but also contributes to faster recovery, reduced risk of complications, and a more positive postpartum experience overall. The findings also emphasize the role of continuous professional development as a strategic component in advancing quality maternal healthcare services.
Strength Points
Several strengths underpin the credibility and significance of this study. The use of a quasi-experimental one-group pretest-posttest design enabled the researchers to measure the direct effect of the educational intervention on the same group of participants, eliminating inter-subject variability. The study’s data collection instruments were validated by a panel of experts and demonstrated high internal consistency, as reflected in strong Cronbach’s alpha scores (0.906 for attitudes and 0.926 for barriers), confirming the reliability of the tools. Another strength is the comprehensive scope of barrier identification. The study categorized barriers into mother-related, nurse-related, physician-related, and system-related factors, providing a nuanced and in-depth understanding of the multi-layered challenges in postpartum pain management. The use of a well-structured, evidence-based educational program with clear, accessible content ensured the intervention was feasible and replicable in similar healthcare settings. Moreover, the statistically significant improvements observed across all domains of attitudes and barrier perceptions highlight the program’s effectiveness and practical relevance.
Limitations
Despite its valuable contributions, the study has several limitations that must be acknowledged. The relatively small sample size of only 20 nurses from a single hospital limits the generalizability of the findings to broader populations or different institutional contexts. The study lacked a control group, which makes it difficult to fully isolate the effects of the intervention from other external factors that might have influenced outcomes. Another limitation is the short-term nature of the post-intervention evaluation. Assessing the participants immediately after the educational program does not provide insights into whether the improved attitudes and reduced barriers are sustained over time. Additionally, the reliance on self-reported data introduces the possibility of response bias, where participants may give answers they believe are expected rather than reflecting their true beliefs or practices. Lastly, the study did not directly assess patient outcomes, such as maternal pain levels or satisfaction, which would provide more concrete evidence of the clinical effectiveness of the intervention.
Conclusion
The study offers compelling evidence that structured educational programs are a powerful tool for improving nurses’ attitudes and minimizing the barriers they face in providing postpartum pain relief. The transformation in attitudes—from largely negative before the intervention to overwhelmingly positive afterward—demonstrates the potential of targeted training to foster meaningful behavioral and perceptual change among healthcare providers. Additionally, the reduction in perceived barriers at all levels—from individual nurse knowledge gaps to systemic institutional constraints—illustrates that education can serve as a catalyst for improving both practice and policy. These findings underscore the critical role of continuous nurse education in enhancing maternal care quality, particularly in resource-constrained settings where postpartum pain is often underrecognized and undertreated.
Based on the study findings, it is strongly recommended that healthcare institutions implement routine, structured educational programs focused on both pharmacological and non-pharmacological pain relief strategies for postpartum mothers. These programs should be embedded within the continuing education framework for nurses and be supported with evidence-based guidelines, standardized pain assessment tools, and updated clinical protocols. Hospitals should also address systemic barriers by improving nurse-to-patient ratios, ensuring adequate time allocation for pain management, and enhancing interdisciplinary communication between nurses and physicians. It is equally important to involve postpartum mothers in educational efforts, empowering them with knowledge about their pain relief options to foster informed decision-making.
Ethical Considerations
The study received ethical approval from the Research Ethics Committee of the Faculty of Nursing, Zagazig University. Official permission was granted by Al-Ahrar Hospital administration. Verbal informed consent was obtained from all participating nurses after explaining the study’s purpose, procedures, and voluntary nature. Confidentiality and anonymity were strictly maintained by using coded data, and participants were assured of their right to withdraw at any time without consequence. No identifying personal data were collected or published.
List of Abbreviations
- NPPR – Non-Pharmacological Pain Relief
- SPSS – Statistical Package for the Social Sciences
- SD – Standard Deviation
- IQR – Interquartile Range
- NPPM – Non-Pharmacological Pain Management
- OCPs – Obstetric Care Providers
- WHO – World Health Organization
- IRB – Institutional Review Board
Acknowledgment
The authors would like to express their deep gratitude to the nursing staff of the postpartum ward at Al-Ahrar Hospital, Zagazig City, for their cooperation, dedication, and valuable participation throughout the study. Special thanks are extended to the hospital administrators and nursing educators who facilitated the implementation of the structured educational program. The authors also appreciate the contributions of data entry assistants and statistical consultants for ensuring accuracy and precision in data analysis. Their collaborative efforts were vital in completing this research.
Author Contributions
- Concept and design: Sabah Lofty Mohamed, Amina Saad Gonied
- Acquisition, analysis, or interpretation of data: Nesreen Zakria Hassan, Sabah Lofty Mohamed, Amina Saad Gonied
- Drafting of the manuscript and critical review for important intellectual content: Amina Saad Gonied, Nesreen Zakria Hassan, Sabah Lofty Mohamed
- Supervision: Sabah Lofty Mohamed, Amina Saad Gonied
Conflicts of Interest
The authors declare that there are no conflicts of interest related to this study or its outcomes.
Confidentiality of Data
All data collected during the research were handled in strict accordance with ethical guidelines and confidentiality protocols as approved by the institutional ethics committee. No identifying personal or patient information was recorded or disclosed in any part of the publication.
Financing Support
This research did not receive any financial support from government bodies, academic institutions, commercial enterprises, or nonprofit organizations.
Financial Relationships
The authors affirm that they have no financial relationships with any organizations or entities that could be perceived to have influenced the submitted work, either presently or within the past three years.
References
- Bishaw, K. A., Sendo, E. G., & Abebe, W. S. (2020). Knowledge, and use of labour pain relief methods and associated factors among obstetric caregivers at public health centers of East Gojjam zone, Amhara region, Ethiopia: a facility based cross-sectional study. BMC pregnancy and childbirth, 20, 1-9.
- Bradfield, Z., Hauck, Y., Kelly, M., & Duggan, R. (2019). “It‟s what midwifery is all about”: Western Australian midwives‟ experiences of being „with woman‟during labour and birth in the known midwife model. BMC pregnancy and childbirth, 19, 1-13.
- Çobanoğlu, A., & Şendir, M. (2019). Evidence-Based Practices in Episiotomy Care. Florence Nightingale Journal of Nursing, 27(1), 48-62.
- Eyeberu, A., Debela, A., Getachew, T., Dheresa, M., Alemu, A., & Dessie, Y. (2022). Obstetrics care providers attitude and utilization of non-pharmacological labor pain management in Harari regional state health facilities, Ethiopia. BMC Pregnancy and Childbirth, 22(1), 389.
- Gallo, R. B. S., Santana, L. S., Marcolin, A. C., Duarte, G., & Quintana, S. M. (2018). Sequential application of non-pharmacological interventions reduces the severity of labour pain, delays use of pharmacological analgesia, and improves some obstetric outcomes: a randomised trial. Journal of physiotherapy, 64(1), 33- 40.
- Heim, M. A., & Makuch, M. Y. (2022). Pregnant women‟s knowledge of non- pharmacological techniques for pain relief during childbirth. European journal of midwifery, 6.
- Karaduman, S., & Akköz Çevik, S. (2020). The effect of sacral massage on labor pain and anxiety: A randomized controlled trial. Japan Journal of Nursing Science, 17(1), e12272
- Osmundson, S. S., Min, J. Y., & Grijalva, C. G. (2019). Opioid prescribing after childbirth: overprescribing and chronic use. Current Opinion in Obstetrics and Gynecology, 31(2), 83-89.
- Rantala, A., Hakala, M., & Pölkki, T. (2022). Women‟s perceptions of the pain assessment and non-pharmacological pain relief methods used during labor: A cross-sectional survey. European Journal of Midwifery, 6.
- Saluja, B., & Bryant, Z. (2021). How implicit bias contributes to racial disparities in maternal morbidity and mortality in the United States. Journal of women’s health, 30(2), 270-273
- Shondell, L., Foli, K. J., & Erler, C. (2020). Effects of education on nurses’ knowledge and attitudes of pain management in a postoperative cardiovascular unit. The Journal of Continuing Education in Nursing, 51(8), 377-383.
- Tabatabaeichehr, M., & Mortazavi, H. (2020). The effectiveness of aromatherapy in the management of labor pain and anxiety: A systematic review. Ethiopian journal of health sciences, 30(3).
- Innab A, Alammar K, Alqahtani N, Aldawood F, Kerari A, Alenezi A. The impact of a 12-hour educational program on nurses’ knowledge and attitudes regarding pain management: a quasi-experimental study. BMC nursing. 2022 Sep 7;21(1):250.
- Ibrahim HA, Alshahrani MS, Al-Qinnah AJ, Elgzar WT. Nonpharmacological pain relief for labour pain: knowledge, attitude, and barriers among obstetric care providers. PeerJ. 2024 Feb 2;12:e16862.
- Ramasamy P, Kwena A, Emarah A, Kangethe S. Knowledge, attitude, practice and barriers to educational implementation of nonpharmacological pain management during labor in selected hospitals, Kenya. Central African Journal of Public Health. 2018 Mar;4(1):20-6.
- Gaber Zagloul M, Saied Hassan S, Ali Abd Elmoaty Sheha E, Elzeblawy Hassan H. Postnatal Evidence Based Nursing Practice: Effect of an Educational Guideline on Internship Student’s Knowledge and Skills. Egyptian Journal of Health Care. 2022 Jun 1;13(2):437-47.