Research
HJOG 2026, 25 (2), 145-155| doi: 10.33574/hjog.0624
Vasilis S. Gavalas
Department of Geography, University of the Aegean, Lesvos, Greece
Correspondence: Vasilis S. Gavalas, Associate Professor, Department of Geography, University of the Aegean, University Hill, Office A.31, Lesvos, Greece Email: bgav@geo.aegean.gr
![]()
Abstract
Greece has one of the highest cesarean section rates in the European Union, far exceeding the 10-15% benchmark recommended by the World Health Organization. This study aims to comprehensively analyze this escalating trend by examining demographic and social factors that influence the delivery method. Using unpublished nationwide data from the Hellenic Statistical Authority (ELSTAT) for 161,152 births in 2021-2022, we explored the spatial distribution of cesarean sections across Greece’s NUTS 2 regions (Nomenclature des Unités Territoriales Statistiques, which is a geographical classification standard established by the European Union (EU)) and applied an aggregated logistic regression to identify key determinants. Our findings reveal a pervasive use of cesarean sections across all regions, with rates consistently above 50%, and peaking at 69% in the Ionian Islands. Statistical analysis confirms that maternal age is the most influential factor, with the odds of a cesarean section increasing dramatically with age. Educational level and family status also play a role, with mothers with a secondary education and those who are married or in a civil partnership showing higher cesarean rates. These findings highlight a critical public health issue and provide an evidence-based foundation for policy interventions aimed at promoting safer, more appropriate obstetric practices in Greece.
Keywords: Cesarean sections, Regions, Age of mother at birth, Educational level, Healthcare providers
Introduction
Cesarean section (C-section for abbreviation) is a surgical procedure used to deliver a baby through an incision made in the maternal abdominal wall and uterus. In ancient times, it was performed only when the woman was dead or dying, as an attempt to rescue the fetus. The first documented C-section on a living woman was performed in 1610, though she died 25 days after the surgery. For centuries, C-sections on living women almost invariably resulted in the mother’s death due to infection (sepsis) and hemorrhage[1]. In the late 19th century with the introduction of anesthesia and antiseptics, the survival rates of both the fetus and the mother improved after cesarean sections, and they were performed when a medical condition required this kind of operation. From the late 20th century C-sections are performed customarily, without medically indicated reasons. In the 21st century, the majority of childbirths are performed with C-section in at least 6 countries (Dominican Republic, Brazil, Greece, Cyprus, Egypt and Turkey), while by 2030 nearly a third of all births are likely to take place by cesarean section worldwide[2].
However, the increasing popularity of cesarean births conceals potential adverse effects on maternal health and on child’s neuropsychiatric development. The relevant literature consistently highlights several negative outcomes associated with C-sections, encompassing both short-term morbidity and long-term complications. In the immediate postpartum period, mothers undergoing C-section are at an elevated risk of various complications compared to those experiencing natural childbirth. From a long-term perspective, cesarean delivery is associated with future subfertility and several subsequent pregnancy risks such as placenta previa, uterine rupture, and stillbirth[3,4].
As far as mortality is concerned, C-sections are commonly associated with higher maternal mortality rates compared to natural childbirth. Nevertheless, it is crucial to understand that directly comparing maternal mortality rates for Cesarean sections and natural childbirths can be complex due to a phenomenon known as “indication bias.” This means that C-sections are often performed in situations where the mother or baby is already at higher risk, meaning the C-section itself is not always the cause of a higher mortality rate, but rather a necessary intervention for a pre-existing complication that could otherwise lead to death. However, even with this caveat, studies consistently show that in developed countries, maternal mortality rates are higher for Cesarean sections. Maternal mortality in developed countries is generally very low, that is below 5 maternal deaths per 100,000 births. Cesarean sections are associated with a 3 to 5 times higher risk of maternal death compared to natural childbirth for low-risk women. A study in the Netherlands showed that in low-risk women the risk of death for C-section is approximately thirteen per 100,000 compared to 3.5 per 100,000 for natural childbirth[5].
In 1985 the World Health Organization (WHO) organized a meeting of reproductive health experts in Fortaleza, Brazil focusing on “appropriate technology for birth”. The key outcome of that meeting was a widely cited statement by a panel of reproductive health experts, setting a benchmark on the cesarean section rates. The statement was that “there is no justification for any region to have a [cesarean section] rate higher than 10-15%”[6]. In 2014 WHO conducted two studies in order to address the need to revisit the 1985 recommended rate. The first study was a systematic review of available studies that had sought to find the ideal cesarean rate within a given country or population, and the second study was a worldwide country-level analysis using the latest available data. Based on these studies WHO concluded once again that “At population level, cesarean section rates higher than 10% are not associated with reductions in maternal and newborn mortality rates”[7]. Moreover, it concluded that Cesarean sections could cause significant and sometimes permanent complications, and they should ideally only be undertaken when medically necessary (ibid).
A significant factor contributing to the rise in C-section rates without a clear medical necessity is the convenience it offers to healthcare providers. A C-section can be scheduled in advance, allowing doctors to manage their time more effectively. Moreover, in many healthcare systems, especially in private hospitals, C-sections are reimbursed at a higher rate than natural deliveries. This creates a financial incentive for both the physician and the hospital to favor surgical delivery[8]. As for the expectant mothers themselves, they may choose a cesarean section for reasons of convenience, whether for scheduling or to avoid the pain of a natural birth[9]. Nevertheless, inadequate information and a lack of informed consent, which can amount to maternal coercion, may constitute a reason for the expectant mother to resort to a C-section. A study in Switzerland revealed that over one-quarter of women (26.7%) reported experiencing some form of informal coercion during childbirth. Women who were pressured or coerced into a C-section are more likely to develop postpartum depression or another mental health disorder[10]. Similarly, an earlier survey conducted in the United States found that 28% of women felt pressured by a clinician to undergo labor induction or a C-section[11].
Greece stands out within the European context for its exceptionally high and continuously rising cesarean section rates. Recent data indicate that Greece’s C-section rate is among the highest in the European Union (62% of all births were delivered with cesarean section in 2022, based on the data sent to the author by ELSTAT), far exceeding the WHO recommendations and the averages of many developed nations. This persistent upward trajectory, despite advancements in obstetric care and increased awareness of the potential downsides of non-medically indicated C-sections, presents a complex public health challenge. The reasons behind this alarming trend are multidimensional, but they may encompass a range of potential factors from an increasing need of C-sections due to the fact that women bear children at increasingly older ages, to pressure from clinicians for cesarean delivery in the absence of clear medical or obstetrical indication.
Despite the critical nature of this issue, comprehensive research specifically exploring the drivers of the increasing C-section rates in Greece remains limited. There are plenty of published papers and very noteworthy students’ dissertations, but the data they use are limited, based mostly on surveys on specific hospitals[12-15]. One published academic paper on cesarean section rates in Greece uses nationwide data on recorded births in 2019-2020 and the authors calculate the C-section rates in the four NUTS1 Regions of Greece (1.Attica, 2.Aegean islands and Crete, 3. Northern Greece, 4. Central Greece). No information on the demographic or social profiles of the mothers are provided, nor an indication as to what extent the cesarean sections were based on medical or obstetrical need[16].
This paper aims to address this critical gap by thoroughly investigating the rates of cesarean sections in Greece down to the level of NUTS 2 Regions and identifying the demographic, educational and social profile of the mothers. By examining demographic, socio-cultural, and systemic factors, this study seeks to provide a comprehensive analysis that can inform evidence-based policy interventions and promote safer, more appropriate obstetric practices.
Material and Methods
Systematic compilation and publication of data on the method of delivery at the national level started only after 2016 in Greece. For this paper, data for two years were requested by the author with a formal petition to ELSTAT[17]. Therefore, ELSTAT sent us data on births for 2021 and 2022 broken down by age of mother at birth, educational level of mother, family status of mother (married, single, in civil partnership), sex of the newborn, method of delivery, and place of permanent residence of mother (NUTS-2 level). In total, 161,152 births were recorded in the two years under consideration, 85,231 in 2021 and 75,921 in 2022. The administrative division of the Greek territory in the NUTS-2 level, as applied by Eurostat, comprises 13 Regions as it can be seen in figure 1. There is also an autonomous area (Mount Athos), which is a monastic community and was excluded from the analysis.
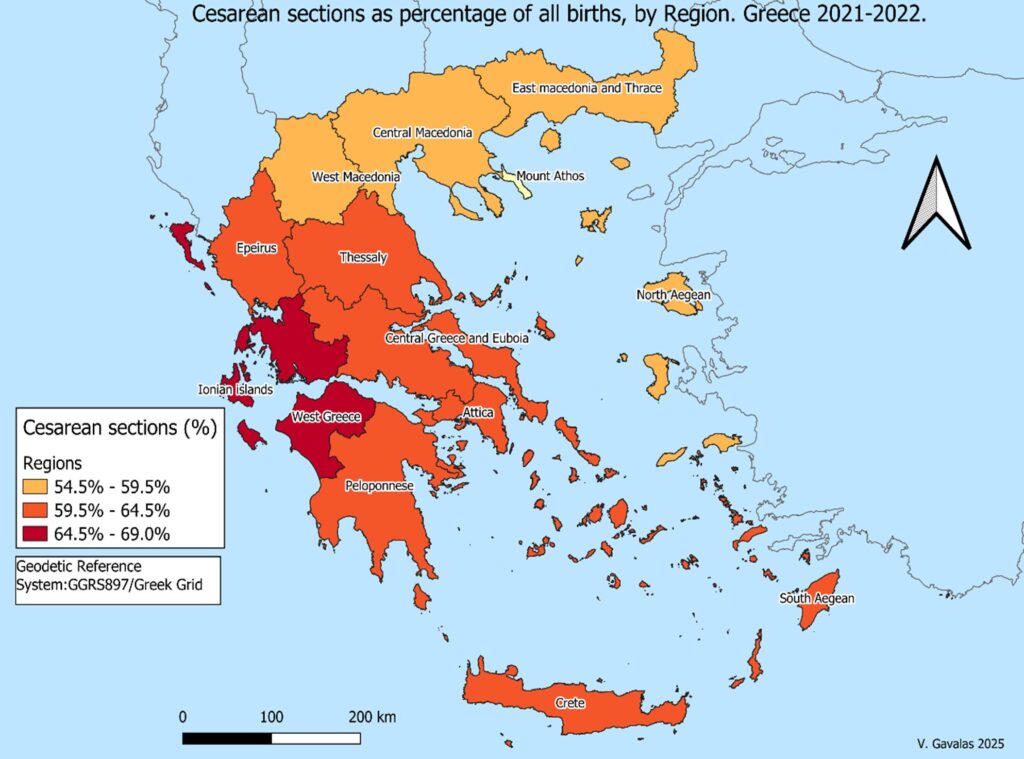
Figure 1. The spatial distribution of C‐section rates in Greece in 2021‐22. Geographical level NUTS 2.
Data processing was performed through the use of the statistical package Stata. Data visualization was accomplished by the use of the GIS program Qgis. The analysis and conclusions are based on descriptive statistics and on multivariate statistical analysis as well. To identify the strongest determinant of the method of delivery (from the socio-demographic variables available), we applied an Aggregated Logistic Regression with Odds Ratios, a specific application of logistic regression. This specific method of logistic regression is designed for use with aggregated data, rather than individual-level data.
Results
The map (Figure 1) reveals a kind of spatial clustering of C-section rates. The western part of Greece (Ionian islands, part of Peloponnese, and Epirus) ap-pears to have the highest percentages (over 62%). Conversely, northern Greece (Thrace, Macedonia, and the North Aegean islands) shows lower rates (54.5% to 59.3%). The rest of Greece, including Attica (the Region encompassing Athens, the capital and biggest urban center of Greece) falls within the intermediate range of 59.5% to 64%. Nevertheless, the differences are relatively small, and the fact is that in every single Region of Greece the majority of births are delivered by cesarean sections. The lowest rate was in West Macedonia (54.7%) and the highest rate was recorded in the Ionian islands (69%).
As it will be clarified further on with the logistic regression, the most influential demographic variable on the method of delivery is the age of mother at birth (Figure 2). The majority of adolescent mothers (56.4%) gave birth with vaginal delivery. This, marginal indeed, preponderance of vaginal delivery among adolescent women may be associated with their socio-economic status. Usually, women at ages below 20 years are of meagre economic condition, and a lot of them are unmarried when they bear their children[18]. Consequently, it is likely that they will choose a public hospital for their childbirth, because the cost is significantly lower than that of a private clinic. Yet, in public hospitals the rates of vaginal deliveries are higher than they are in private clinics[13,15]. It is plausible, therefore, that the lower rate of C-sections (43.2%) among adolescent mothers in Greece, might have to do with the different rates between public and private hospitals, and is not correlated with the age of mother. However, this is only a working Hypothesis, and it needs further research to be verified (or discharged).

Figure 2. Method of delivery by age of mother. Greece, 2021‐2022. Source: Unpublished data provided by ELSTAT (own elaboration). N=161152 live births.
Note: vaginal deliveries comprise both spontaneous deliveries (natural childbirth) and vaginal deliveries after induced labor.
The data at hand show that as the age of mother progresses the rates of C-sections are increasing (Figure 2). From the age of 20-24 the majority of deliveries (53.3%) take place with a C-section, while this rate reaches 94% at the ages of 45+. This means that it is extremely rare for a woman in Greece to bear a child without a cesarean section if she is above 45 years of age.
Another determinant of the method of delivery is the educational level of the mother (Figure 3). The most likely women to resort to a cesarean section are those who have graduated from the secondary or post-secondary education (which in Greece comprises vocational and training schools after high school). The percentage of women of this educational level who gave birth through C-section was 64.1%. Illiterate or of low literacy women are less likely to resort to a C-section, maybe because their low educational level is associated with a lower economic status and their choice of a public hospital for the childbirth. University graduates and above are in-between, with the rate of C-sections being 60.5% among them.
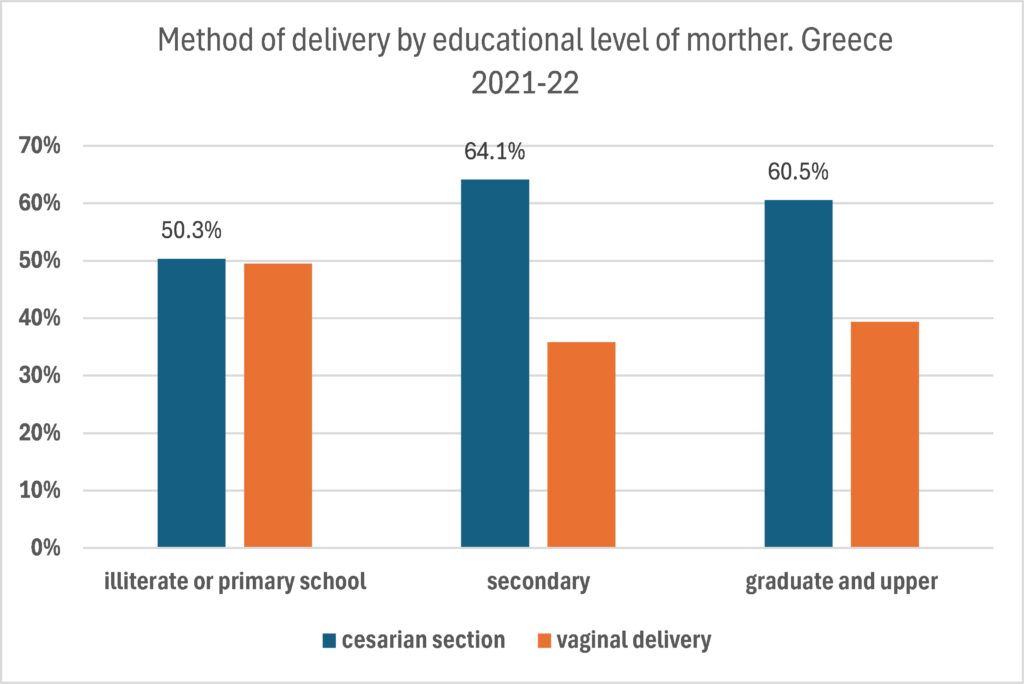
Figure 3. Method of delivery by educational level of mother. Greece 2021‐2022. Source: Unpublished data provided by ELSTAT (own elaboration). N=161152 live births. 8493 women do not declare their educational level.
Family status of the mother is associated with variations in the delivery method, as well. Data indicate (figure 4) that C-section rates are highest among mothers who are married or in civil partnerships (62%), and lower for unmarried mothers (56%). A possible explanation for this disparity is the age difference between these groups, as unmarried mothers are, on average, younger[16]. This demographic trend may influence delivery outcomes, as younger mothers typically experience fewer complications that necessitate a cesarean section. Furthermore, socioeconomic factors may play a role; unmarried mothers, who often face greater financial disadvantage, may be more likely to deliver in public hospitals, where the overall rate of Cesarean sections is lower.
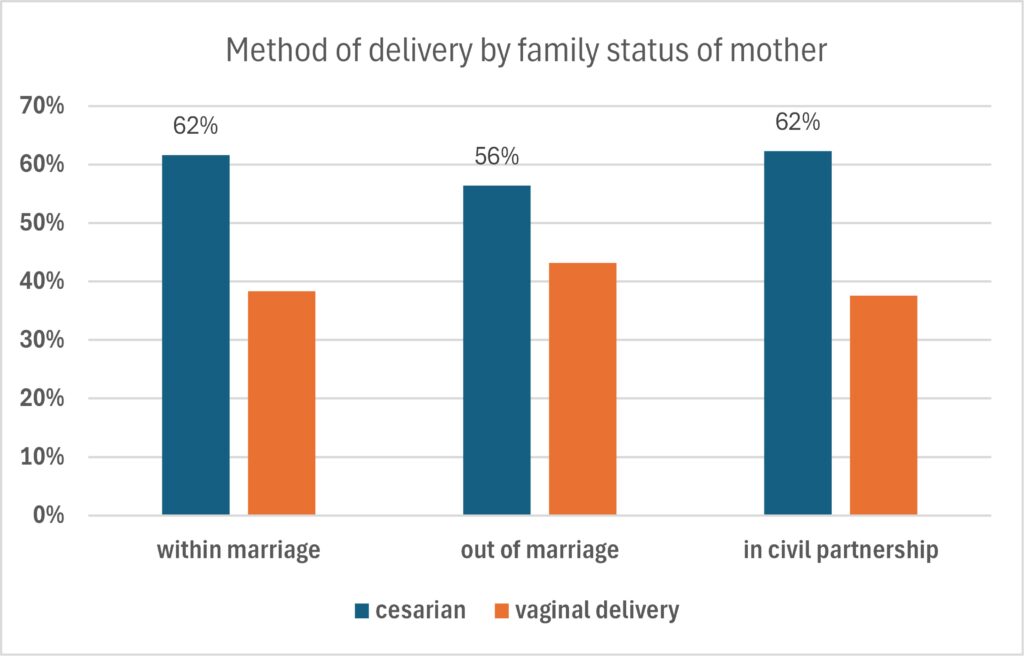
Figure 4. Method of delivery by family status of mother.
Finally, the sex of the newborn does not appear to be a significant factor in determining the method of delivery. While C-section rates were marginally higher for male births (61.7%) compared to female births (60.6%), this difference is statistically negligible (Figure 5).
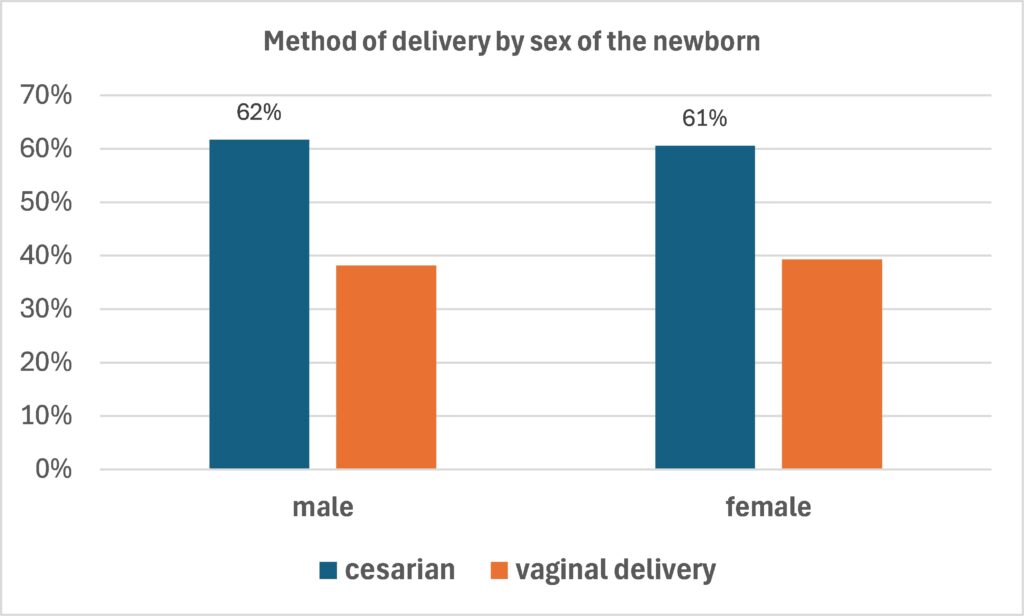
Figure 5. Method of delivery by sex of the newborn.
Source: Unpublished data provided by ELSTAT (own elaboration). N=161152 live births.
Table 1 shows a statistical model that examines how social and demographic factors influence the likelihood of a woman having a cesarean section. The value labels of the variables included in the statistical model are displayed in table 2. The model includes three independent variables (age, educational level, and family status of the mother) and one dependent variable (method of delivery). When many parameters are fitted to the model it is inevitable that there will be an “interaction effect”, that is the relationship between an independent variable (predictor) and the dependent variable changes depending on the value of another predictor variable. For example, in our model, the family status of the mother may interact with age and educational level. Unmarried mothers in Greece tend to be of young age and of low educational level[16]. Moreover, the more predictors are fitted to the model, the greater the amount of chance error will be. Therefore, we should pay attention to the level of statistical significance to ensure that the outcome would not arise by random chance or by interaction effect.
In interpreting the results of table 1, one should first observe how well the model fits our data (Model Fit). The chi-squared value (χ2(11)=4705.26) with a p-value< 0.001 indicates that the overall model is statistically significant. This means that at least one of the predictor variables (age, education, or family status) is associated with the dependent variable (method of delivery) in a non-random way. The Pseudo R2 of 0.0219 suggests that the predictors in this model explain about 2.2% of the variation in the outcome (method of delivery). While this value seems low, it is common for models with a large sample size and can still be practically meaningful.
The omitted categories are age1 (15-19), education1 (illiterate, or primary school), family status1(within marriage). This is the basis for interpreting the results of the logistic regression. Therefore, the baseline is an adolescent illiterate married woman. For example, the determinant “Iage_2” is associated with an odds ratio of 1.36, meaning that a woman aged 20-24 is 1.36 times more likely to have a childbirth with C-section than a woman aged 15-19, all other factors (educational level and family status) being equal. It seems that age is the most important of the three factors in the likelihood of a woman having a C-section. A woman aged 45+ (Iage_7) is 22.8 times more likely to have a C-section than her adolescent counterpart.
The educational level of the mother also plays a role in determining the method of childbirth. It seems that mothers with a secondary or post-secondary school education have approximately 1.36 times higher odds of having a cesarean section compared to mothers who are illiterate or have low literacy, all other factors (age and family status) being equal, and this outcome is statistically significant at α=0.05. However, results for university graduates and over (“Ieducatio_3”) and for women who did not declare their educational level (“Ieduca_4”) are not statistically significant at 0.05 level of significance. As far as the family status of the mother is concerned, there seems to be an interaction effect of unmarried mothers (Ifamily_2) with age and education. That is why table 1 indicates that unmarried mothers have a slightly higher odds ratio for a cesarean section (1.04) compared to married mothers, while in reality the percentage of unmarried mothers who resorted to C-section was lower than that of married ones (figure 4). To disentangle any kind of interaction effect, table 3 presents the association between family status and method of delivery, without any other independent variables added in the model.
It is clear from table 3 that unmarried mothers (“Ifamily_2”) are less likely to resort to a C-section than married ones (“Ifamily_1”). Results for those in civil partnership (“Ifamily_3”) are not statistically significant at the a=0.05. As it was mentioned above, women in civil partnership have about the same chances of having a C-section as the married ones.
Discussion
This study investigated the escalating rates of cesarean sections in Greece, a trend that has surpassed WHO recommendations and the averages of many developed nations. Our analysis, utilizing data from 2021-2022 across Greek regions, confirms the pervasive nature of C-sections, with the majority of births occurring via this procedure in every Region of Greece. While regional variations exist, with the Ionian Islands exhibiting the highest rates (up to 69%) and West Macedonia the lowest (54.7%), the overarching finding is the widespread adoption of C-section.
Examination of demographic factors shed light on key determinants of this trend. Maternal age emerged as the most significant predictor. Adolescent mothers (15-19 years) demonstrate a higher propensity for natural delivery (either entirely natural or after induced labor), a phenomenon that may be influenced by socioeconomic status and a higher likelihood of opting for public hospitals, which, as indicated, tend to have lower C-section rates. Conversely, as maternal age advances, the likelihood of a cesarean section increases dramatically. For women aged 45 and over, the C-section rate reaches an astonishing 94%, highlighting a critical shift in delivery practices for older mothers.
Educational attainment also plays a role, though its impact is not straightforward. Women with secondary education exhibited the highest C-section rates (64.1%). It is plausible that this group may be more susceptible to physician intimidation and less likely to advocate for alternative delivery methods. Conversely, women with poorer literacy levels showed lower C-section rates, which might be due to economic constraints leading them to utilize public healthcare systems. University graduates and above fell in an intermediate range, suggesting a complex interplay of factors, potentially including a greater ability to critically assess medical advice and advocate for their preferences.
Family status also demonstrated a correlation with C-section rates, with married or in-civil-partnership mothers showing higher rates (62%) compared to unmarried mothers (56%). This disparity could be partly explained by the younger average age of unmarried mothers, aligning with the observed trend of lower C-section rates in younger age groups. Socioeconomic factors for unmarried mothers, potentially including greater financial challenges, might also contribute to a higher utilization of public hospitals, where C-section rates are generally lower.
The statistical model confirmed that age, educational level, and family status are significant determinants of the method of delivery. Notably, age was the strongest predictor, with women aged 45+ being 22.8 times more likely to have a C-section than adolescent mothers. The relatively low Pseudo R-squared of 0.0219, while indicating that these variables explain a small proportion of the variation, is common in large datasets and still allows for practical interpretation. The identified interaction effects, although not fully explored in this analysis, suggest that these demographic factors do not operate in isolation and their combined influence on delivery method warrants further investigation.
In concluding, the cesarean section rate in Greece was reported to be 62% in 2022. This figure is substantially higher than the 10-15% benchmark established by the World Health Organization (WHO), a rate beyond which there is no evidence of improved maternal or neonatal outcomes. Consequently, the high prevalence of cesarean deliveries in Greece suggests that in their great majority these procedures are medically unnecessary. The persistent upward trend in C-section rates, even in the absence of clear medical indications, is concerning, given the documented potential adverse effects on maternal and infant health. The increasing utilization of C-section without medical necessity not only exposes women to potential short-term morbidities like hemorrhage and wound complications but also long-term risks such as future subfertility and complications in subsequent pregnancies.
Evidence-based policy interventions are urgently needed to promote a more judicious use of C-sections, emphasizing natural childbirth when medically appropriate, and ensuring that all delivery decisions are guided by the best interests of maternal and infant well-being. This may involve targeted public health campaigns, enhanced prenatal education, and a review of current obstetric protocols and incentives to encourage safer and more appropriate delivery practices.
Disclosure of Conflicts of Interest
The author reports no conflicts of interest.
References
- Encyclopedia Britannica. Cesarean section. In: Britannica [Internet]. [cited 2025 Jul 10]. Available from: https://www.britannica.com/science/cesarean-section
- World Health Organization. Caesarean section rates continue to rise, amid growing inequalities in access [Internet]. Geneva: World Health Organization; 2021 [cited 2025 Jul 10]. Available from: https://www.who.int/news/item/16-06-2021-caesarean-section-rates-continue-to-rise-amid-growing-inequalities-in-access
- Sandall J, Tribe RM, Avery L, Mola G, Visser GH, Homer CS, et al. Short-term and long-term effects of cesarean section on the health of women and children. Lancet. 2018;392(10155):1349-1357.
- Keag OE, Norman JE, Stock SJ. Long-term risks and benefits associated with cesarean delivery for mother, baby, and subsequent pregnancies: Systematic review and meta-analysis. PLoS Med. 2018;15(1):e1002494.
- Kallianidis AF, Schutte JM, Van Roosmalen J, Van Den Akker T. Maternal mortality after cesarean section in the Netherlands. Eur J Obstet Gynecol Reprod Biol. 2018;229:148-52.
- World Health Organization. Appropriate technology for birth. Lancet 1985;2:436-7.
- World Health Organization. WHO statement on cesarean section rates [Internet] IRIS [cited 2025 Jul 10] Available from: https://iris.who.int/handle/10665/161442
- Matsagganis M. The economics of obstetric services in Greece [in Greek]. Athens: Kritiki publications; 2001.
- Ntara A. Frequency of cesarean section in Greece and socioeconomic factors that affect it [in Greek] [Bachelor’s dissertation]. Kalamata: TEI Kalamatas; 2015.
- Oelhafen S, Trachsel M, Monteverde S, Raio L, Cignacco E. Informal coercion during childbirth: risk factors and prevalence estimates from a nationwide survey of women in Switzerland. BMC Pregnancy Childbirth. 2021;21(1):369.
- Jou J, Kozhimannil KB, Johnson PJ, Sakala C. Patient-perceived pressure from clinicians for labor induction and cesarean delivery: a population-based survey of US women. Health Serv Res. 2015;50(4):961-81.
- Roussi A. Cesarean: heavy industry in Greece [in Greek] [Master’s thesis]. Piraeus: University of Piraeus; 2008.
- Dionissopoulou GN. The issue of cesarean sections in Greece [in Greek] Master’s thesis. University of Piraeus; 2014.
- Mossialos E, Allin S, Karras K, Davaki K. An investigation of Cesarean sections in three Greek hospitals: the impact of financial incentives and convenience. Eur J Public Health. 2005;15(3):288-95.
- Kouimtsidou S, Solakidou A. The problem of cesarean sections in Greece and the role of the midwife [in Greece] [Doctoral dissertation]. Kozani: TEI of Western Macedonia; 2020.
- Kontopanos A, Tsakiridis I, Dagklis T, Boureka E, Mamopoulos A, Athanasiadis A. Cesarean section rates in each region of Greece: A retrospective analysis. HJOG. 2023;22(1):35-44.
- ELSTAT. Dataset on births for 2021 and 2022 broken down by various socio-demographic variables and method of delivery (tailor-made upon request). Athens: ELSTAT; 2025.
- Gavalas VS, Raftakis M. Redefining family structures: Births out of wedlock in 21st century Greece. Popul Space Place. 2024;30(8):e2806.