Review
HJOG 2026, 25 (3), 255-270 | doi: 10.33574/hjog.0634
Georgios Sourlas1, Konstantinos Pantazis2, Menelaos Lampropoulos1, Angelos Daniilidis3
1Department of Gynaecology, Agios Demetrios General Hospital of Thessaloniki, Greece
22nd Department of Obstetrics and Gynaecology, Department of Medicine of Aristotle University of Thessaloniki, Hippokrateion Hospital of Thessaloniki, Greece
31st Department of Obstetrics and Gynaecology, Department of Medicine of Aristotle University of Thessaloniki, Papageorgiou Hospital of Thessaloniki, Greece
Correspondence: Dr. Georgios Sourlas, 80 Vasileos Konstantinou Street, 56728 Thessaloniki, Greece, Tel.: +306949813013, e-mail: sourlasgeorge16@gmail.com
![]()
Abstract
Objective: Ovarian ectopic pregnancy is a rare but potentially life-threatening condition that may lead to severe hemorrhage if misdiagnosed or left untreated. Reported frequency of ovarian pregnancy is 0.5%–1% of all extra-uterine gravidities, accounting for about 0.5–3% of all ectopic pregnancies. This scoping review aimed to evaluate the current role of laparoscopy in the treatment of ovarian pregnancy.
Materials and Methods: A comprehensive search of PubMed, Web of Science and Epistemonikos was carried out for publications within a range from January 2012 until December 2025. Inclusion criteria were records published in English, referring to a target population of female patients with clinical, laboratory and ultrasonographic findings of ovarian pregnancy who underwent laparoscopic treatment. The methodology framework proposed by Arksey and O’Malley was used to guide the scoping review process, which adhered to PRISMA-ScR guidelines.
Results: The search process resulted in 45 publications reporting on laparoscopic management of ovarian pregnancy. These were focused on the efficacy and safety of laparoscopic treatment of ovarian pregnancy, the different types of laparoscopic approach, comparison between the management options of laparoscopy and laparotomy and postoperative fertility outcome. The preferable and commonest laparoscopic procedures are those that allow ovarian-sparing, which include enucleation of the gestational sac and ovarian wedge resection, whereas laparoscopic adnexectomy is the last resort for patients with significant hemodynamic instability. Laparoscopy appears to outweigh laparotomy, presenting significant advantages over open surgery. Post-operative fertility outcomes among patients who wish to maintain their reproductive potential do not seem to be compromised in the case of laparoscopy.
Conclusions: Laparoscopy constitutes the gold standard for the management of ovarian pregnancy, with a high rate of successful removal and uneventful recovery among treated patients.
Key words: Ovarian pregnancy, laparoscopy, fertility outcome, scoping review
Abbreviations: OP= ovarian pregnancy, TP= tubal pregnancy, EP= ectopic pregnancy, IUP= intrauterine pregnancy, OWR= ovarian wedge resection, ART= assisted reproductive technology, IVF= in vitro fertilization
Introduction
Ovarian pregnancy (OP) is a rare type of non-tubal ectopic pregnancy in which the gestational sac is implanted, grown, and developed in the ovary. Its incidence is approximately 0.5%–3% of ectopic pregnancies, accounting for 1/7000–1/40,000 live births. With the development of assisted reproductive technology (ART) techniques, the incidence of OP has been increasing, consisting up to 0.3% of all in vitro fertilization (IVF) pregnancies and 6% of all IVF ectopic pregnancies. This rise is also reported due to the evolution of transvaginal ultrasonography and careful histologic examination of ovarian tissues1.
Ovarian pregnancy consists a potentially life-threatening gynecological emergency, occurring primarily during the 1st trimester of pregnancy2-3. Not rarely, it clinically manifests as hemoperitoneum because of the diagnostic delay and the rupture of this rich in vascularization ectopic lesion. Its preoperative diagnosis is challenging because it morphologically and ultrasonographically mimics a corpus luteum cyst, an ovarian tumor or a tubal pregnancy4. That is why pre-operative confirmation of OP remains a constant challenge, with the majority of cases diagnosed intraoperatively, along with pathologic evidence of gestational product implantation or attachment on ovarian tissue2.
Surgery constitutes the principal treatment for OP, with methotrexate treatment remaining controversial. With the continuous development of minimally invasive surgery, laparoscopy has gradually become the most frequently used method for OP treatment, presenting significant advantages compared to laparotomy, like shorter hospital stay, faster recovery and less postoperative adhesions. Although ipsilateral oophorectomy was the preferred procedure in the past, more conservative ovarian-sparing techniques, such as removal of gestational products or ovarian wedge resection, have now become the most suitable management approaches for OP patients who wish to preserve their fertility5.
This scoping review aims to evaluate the role of laparoscopy as the gold standard method of OP treatment, while focusing on its efficacy and safety, the different laparoscopic approaches, especially the ones corresponding to ovarian-sparing surgery, its advantages over laparotomy and the postoperative fertility outcome as reported in current literature.
Materials and methods
In order to ensure consistency and transparency of the scoping review, this study adhered to the “PRISMA extension for scoping reviews” (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews), which is a good practice checklist that was developed by a 24-member expert panel and 2 research leads following published guidance from the EQUATOR (Enhancing the Quality and Transparency Of Health Research) Network and reported by Tricco et al.6. The methodological framework was previously reported by Arksey and O’Malley7. PRISMA-ScR was used with the intent of enhancing transparency and completeness, as it helps with developing a greater understanding of the relevant terminology, the core concepts and the key items of this scoping review.
Data sources and search strategy
In order to construct the research question and organize the search of the literature, “PCC” framework model was utilized (Population, Concept, Context)6. A comprehensive search of PubMed, Web of Science and Epistemonikos was performed from January 2012 until December 2025. The search focused on the efficacy and safety of laparoscopic treatment of OP, the different types of laparoscopic approach, reports comparing laparoscopy to laparotomy, as well as reports mentioning postoperative fertility outcome. The search query terms utilized were: (ovarian pregnancy) AND (laparoscopy).
Study selection-inclusion/exclusion criteria
Studies that were included for this scoping review involved female patients with clinical, laboratory and ultrasonographic findings of intact or ruptured OP who underwent laparoscopic treatment. The time interval of the studies was from January 2012 until December 2025. The type of studies included was one of the following; case report, case series, review, literature review, systematic review, clinical analysis, retrospective analysis, retrospective review, retrospective case-control study and guideline. Articles describing cases of heterotopic or bilateral OP were also included.
Articles not mentioning or examining at all laparoscopic treatment of OP, articles mentioning cases treated only by laparotomy, or articles referring only to medical treatment of OP, were excluded. Finally, literature search was restricted to English language, including articles that have been translated to English, whereas reports written in different languages were excluded.
Data extraction
Review process was divided in 2 stages and screening of articles was contacted via “Rayyan” systematic review management platform. In the 1st stage, duplicate reports were successfully removed. Afterwards, titles and abstracts were screened. Only abstracts that were relevant with the PCC outline were included. In the 2nd stage, only English language full-text reports that could be retrieved were reviewed and further filtering was achieved. A scoping synthesis of the results was opted due to heterogeneity of the included studies and the nature of their findings.
Outcomes
The primary outcomes of this scoping review were the efficacy and safety outcomes in the included reports for the 3 laparoscopic approaches described, as well as the comparison between laparoscopy and laparotomy. The latter included parameters like intraoperative blood loss, length of hospital stay and postoperative complications. Additionally, postoperative fertility outcome was included for the cases where fertility preservation was of interest.
Results
General characteristics
Of the 1545 imported references, 1052 articles were included in the 1st stage of the scoping review. Only full-text articles were reviewed. At the end of the 2nd stage, a total of 45 reports were included. The Flow Diagram of included studies is shown in Figure 1. These reports consisted of 35 case reports, 1 case series, 7 literature reviews, 3 reviews, 2 retrospective reviews, 1 systematic review, 2 retrospective analysis, 2 clinical analysis, 2 retrospective case-control studies and 1 guideline (combination also occurred). Table 1 in Appendix section describes in detail their study design, interventions, outcomes and main conclusions.
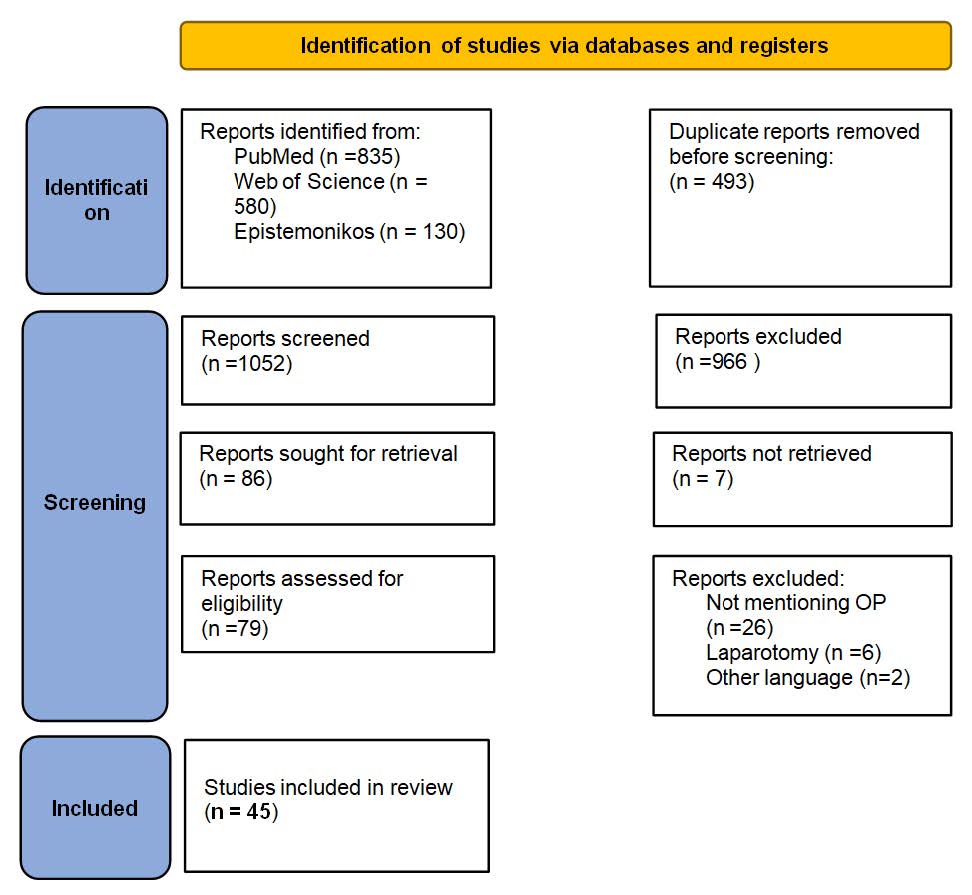
Figure 1. Flow Diagram of studies included in scoping review.
Laparoscopic enucleation of gestational OP sac
Many authors5,8-18 reported on treating both ruptured and intact OPs by enucleating them and preserving as much healthy ovarian tissue as possible. Qing et al.19, after enucleation of the OP and management of hemoperitoneum, administered 50mg of methotrexate locally. Some authors decided to suture the ovaries after enucleation of the gestational OP sac20-23. Aoyagi et al.4 reported on concomitant enucleation of a co-existing ipsilateral endometrioma at the time of the enucleation of OP. Tambimuttu et al.24 reported on concomitant treatment of a contralateral hemorrhagic corpus luteum at the time of the resection of hemorrhagic OP. In addition, other authors25-27 reported the first cases of primary or secondary heterotopic ovarian pregnancies managed effectively with the same technique. More specifically, Hong et al.26 performed an emergency single-port access laparoscopic surgery for rapid management of the rupture. Furthermore, Lee et al.28 reported one rare case of bilateral OP resection after failure of methotrexate treatment, whereas others29-31 reported on ovary sparing OP resection combined with salpingectomy for the treatment of co-existing TP & OP, located at the opposite or the same adnexa.
Laparoscopic ovarian wedge resection
Ovarian wedge resection (OWR) by laparotomy was the treatment of choice until 1990, followed by laparoscopy thereafter32. Feit et al.33 found ovarian wedge resection and bilateral salpingectomy effective for managing a ruptured OP. Similarly, many authors reported successful ectopic lesion removal and hemoperitoneum control by applying the same technique17,34-35. In addition, some authors preferred OWR for resecting a heterotopic OP without risking the ongoing development of the intrauterine pregnancy36. Also, it has been stated that OWR resulted to uneventful recovery for patients with primary OP (patients without history of infertility or ART treatment)37. Certain authors decided to suture the affected ovary after OWR in order to secure proper hemostasis38-39. There is generally only 1 reported guideline in the literature suggesting that clinicians are allowed to perform laparoscopic OWR rather than oophorectomy for OPs, only if they consider it clinically appropriate40. In 1 larger study, it is also evident that OWR is the laparoscopic approach of choice in the majority of cases3. In the retrospective analysis of Wong et al.2, OWR was the preferred procedure, except for the cases that required only gestational sac enucleation due to superficial attachment of the conceptus without involvement of the ovarian cortex.
Laparoscopic adnexectomy
Certain authors have suggested adnexectomy as the last resort for the laparoscopic management of complicated OP, especially in patients with hemodynamic instability41 or with uncontrollable bleeding42. In particular, Stanley et al.43 reported on a case of a ruptured heterotopic ovarian pregnancy, in which they decided to proceed to laparoscopic partial oophorectomy, with successful management of the ectopic pregnancy but with the intrauterine pregnancy resulting to a missed abortion. In a similar manner, Dunphy et al.44 performed laparoscopic oophorectomy with bipolar diathermy for a ruptured OP. Hasegawa et al.45 chose laparoscopic salpingo-oophorectomy in a case of serious active bleeding involving more than one third of the ovarian cortex, as they faced significant difficulty to preserve patient’s adnexa with OWR. In a single case of a ruptured ovarian molar pregnancy, partial oophorectomy by Obeidi et al.46 proved successful in treating the ectopic lesion, as well as the subsequent hemoperitoneum. Additionally, M. Sueldo et al.47 reported a rare case of concurrent OP and ipsilateral TP after a double embryo transfer, which required an OP removal and an ipsilateral salpingectomy respectively. Despite the fact that laparoscopic ipsilateral oophorectomy is effective and definitive treatment, it is becoming less common because of the benefits of ovarian-sparing techniques like OWR and enucleation of gestational sac38. In a similar manner, because laparoscopic salpingectomy can affect ovarian blood supply, thus being detrimental to fertility potential, the majority of authors remain in favor of more conservative techniques17.
Laparoscopy vs Laparotomy
There are not enough reports in current literature comparing laparoscopy to laparotomy regarding surgical treatment of OP, although a trend towards laparoscopic surgery for OP has become apparent. It has been reported that there were no significant differences in operation time or intraoperative blood loss between laparoscopic surgery and laparotomy for OP5. However, shorter hospital stay and lower rate of post-operation pyrexia were found in patients who underwent laparoscopic surgery. In general, it was preferred to treat more advanced pregnancies with laparotomy or/and adnexectomy41.
Post-operative fertility outcome
Due to the rarity of OP, not enough studies exist in current literature regarding post-operative fertility outcome of OP patients that received laparoscopic treatment. In some case reports, patients with uneventful recovery were able to successfully conceive postoperatively, either naturally or via IVF21,23,37. Furthermore, Shao et al.5 in a 3-year follow-up of 49 patients with fertility desire, revealed that 24 of them conceived spontaneous IUPs, 5 conceived IUPs via ART, 2 had EPs, and 18 failed to conceive. Between laparoscopy and laparotomy, no statistically significant differences in reproductive outcomes were found. In addition, Le et al.17 in a 3-year follow-up of 42 cases, mentioned that 26 cases were pregnant at 1 year after surgery, of which 23 cases had IUP and 3 cases had TP. Additionally, 4 cases were pregnant at 3 years after surgery (of which 2 cases were diagnosed as secondary infertility) and 10 cases were diagnosed with infertility pre-operatively and failed to conceive post-operatively. Lower rates of EP and infertility were observed in re-pregnancy, indicating that their results were comparable with other types of EP. Last but not least, in the retrospective analysis of Wong et al.2, during the 3-year observational period, no case of recurrent OP was reported and subsequent spontaneous IUP was observed in 13 out of 21 patients, either naturally or via ART treatment, with an overall pregnancy rate of 71.43%. However, 6 women failed to conceive, with only 2 of whom suffering from unexplained infertility. Authors hypothesized that patients after laparoscopic treatment of one episode of OP present favorable reproductive outcomes and similar reproductive complications to those receiving laparoscopic treatment for TPs or other adnexal pathologies.
Discussion
This scoping review aimed at evaluating the role of laparoscopic surgery as the gold standard of treatment for OPs and elucidate its effectiveness and safety in OP resection and successful management of hemoperitoneum, as well as the advantages over laparotomy in the majority of cases. Healthy ovarian tissue preservation is highly advised and should be sought after in patients who wish to preserve their fertility. Recurrence of OP after successful laparoscopic removal is rare and no such case has been reported yet the literature. Regarding fertility outcome after laparoscopic management, there is no significant decrease in terms of clinical pregnancy and live birth rates2,5.
Without any doubt, the advantages of laparoscopic treatment of OP become apparent both in the diagnostic and the treatment context. In particular, laparoscopy reveals the exact extend of ovarian cortex that is occupied by the ectopic lesion and confirms the suspected rupture of OP. So, its minimally invasive role in diagnosis is more accurate than transvaginal ultrasonography, especially when the ultrasonographic findings are confusing and disorientating. Compared to laparotomy, the superiority of laparoscopy becomes apparent intraoperatively, as it requires less operative time, it is associated with lower blood loss, shorter hospital-stay and faster discharge and is, therefore, more cost-effective. Laparoscopy, also, requires less postoperative analgesia, it possibly comprises lower risk of pelvic adhesions and finally provides better visualization of the operative field. One should not forget that hemodynamic instability is not an absolute contraindication for laparoscopy because it has been proven successful in managing even large amounts of hemoperitoneum24,27.
When it comes to deciding which laparoscopic approach one should follow for OP resection, fertility desire is a critical parameter in deciding on surgical planning. Based on this scoping review, we can claim that among the 3 laparoscopic approaches described in current literature, enucleation of the gestational sac of OP is superior to ovarian wedge resection (which in turn is superior to adnexectomy), as it preserves larger amount of ovarian cortex, rendering this technique the most conservative in treating OP. In general, healthy ovarian tissue sparing may allow not only the possibility for natural conceptions, but also the opportunity for future oocyte retrieval, resulting to subsequent successful pregnancies for patients requiring ART treatment for primary or secondary infertility39. Nevertheless, many authors didn’t always clarify why they chose one method instead of the others, therefore larger future studies should focus on the impact of each ovarian-sparing technique on fertility potential.
Postoperative reproductive outcomes after laparoscopic treatment of OP are influenced by the extent of surgical manipulation and thermal injury during operative laparoscopy, which put healthy ovarian tissue into direct or indirect danger of harm. In particular, monopolar or bipolar electrocoagulation, which are frequently used to control bleeding and provide effective hemostasis, have been found to reduce ovarian vascularization and the number of healthy follicles, causing therefore an irreversible reduction in ovarian reserve48-50. However, authors do not seem to be very concerned about the future reproductive potential of patients undergoing laparoscopic treatment of OP2.
The present scoping review shows some limitations. More specifically, the available current literature about the management of OP mostly consists in case reports, case series, and retrospective studies. Randomized controlled trials, systematic reviews or meta-analyses have not been conducted yet due to the rarity of OP incidence and because of the difficulty of pre-operative diagnosis of this specific ectopic lesion. In addition, it is highly probable that cases with favorable outcome are more likely to be reported and published, resulting to a possible percentage of bias when it comes to success and safety of laparoscopic management of OP, combined with successful postoperative reproductive outcome. This may also explain the high success and minimal complications rates of laparoscopic treatment of OP reported by several authors. One should keep in mind that because of the high rate of misdiagnosis of OP due to similar ultrasonographic manifestations to TP or corpus luteum, several cases may have been missed. Furthermore, the case reports that were retrieved might have been influenced by the level of clinical experience, available resources, heterogeneous case presentations, different surgical skillset and methodologies each surgeon offers, combined with each surgeon’s familiarity to certain laparoscopic approaches, thus rendering the comparison of cases significantly difficult. It is also worth mentioning that not enough reports in current literature clarify the criteria that have to be met in order to make the most suitable treatment choice between laparoscopy and laparotomy, or even between laparoscopy and methotrexate treatment. Additionally, not many reports include long term follow-up and fertility monitoring after laparoscopy, which is essential in order to compare the impact of the different methods on fertility.
Conclusion
The rarity and ultrasonographic resemblance of ovarian pregnancy with other adnexal pathologies make the preoperative diagnosis of this type of ectopic pregnancy challenging. Laparoscopy constitutes not only the most accurate method for establishing the definite diagnosis of ovarian pregnancy, but also the gold standard for treating it effectively and safely. The reproductive prognosis of OP patients that were treated laparoscopically is favorable and encouraging. However, more research is needed in order to reveal which laparoscopic technique is preferable when it comes to healthy ovarian tissue preservation, particularly in view of the fact that patients with OP are often already affected with infertility and it is in their high interest to preserve their fertility potential.
Contribution statement
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Georgios Sourlas and Konstantinos Pantazis. The writing was done by Georgios Sourlas and Konstantinos Pantazis and all authors contributed in the editing. All authors approved the final submitted manuscript.
Funding
The authors received no external funding for this work.
Declaration of competing interest
The authors declare that they have no conflict of interest regarding the publication of this scoping review.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary material. Raw data that support the findings of this study are available from the corresponding author, upon reasonable request.
References
- Ge L, Sun W, Wang L, Cheng L, Geng C, Song Q, Zhan X. Ultrasound classification and clinical analysis of ovarian pregnancy: a study of 12 cases. Journal of gynecology obstetrics and human reproduction. 2019 Nov 1;48(9):731-7. https://doi.org/10.1016/j.jogoh.2019.04.003
- Wong CH, Wang YL, Huang JP. Postoperative reproductive outcomes in women with ovarian pregnancy: a retrospective analysis. Taiwanese Journal of Obstetrics and Gynecology. 2021 Mar 1;60(2):295-8. https://doi.org/10.1016/j.tjog.2021.01.007
- Li H, Liu Y, Yang Y, Zhao X, Qi X. Clinical analysis of women with ovarian pregnancy: a retrospective case–control study. BMC Pregnancy and Childbirth. 2022 Oct 13;22(1):768. https://doi.org/10.1186/s12884-022-05099-8
- Aoyagi Y, Kai K, Aso S, Nishida M, Kawano Y. Coexistence of Ovarian Endometrioma and Ovarian Pregnancy: A Case Report. Cureus. 2023 Feb 28;15(2).https://doi.org/10.7759/cureus.35608
- Shao M, Wang X, Zhou X. Case Report: Ovarian pregnancy, a rare but lethal condition: An analysis of 112 cases. Frontiers in Surgery. 2023 Feb 17;10:1062228.https://doi.org/10.3389/fsurg.2023.1062228
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, Moher D, Peters MD, Horsley T, Weeks L, Hempel S. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Annals of internal medicine. 2018 Oct 2;169(7):467-73.https://doi.org/10.7326/m18-0850
- Arksey H, O’malley L. Scoping studies: towards a methodological framework. International journal of social research methodology. 2005 Feb 1;8(1):19-32. https://doi.org/10.1080/1364557032000119616
- Wu B, Li K, Chen XF, Zhang J, Wang J, Xiang Y, Zhou HG. Ovarian pregnancy rupture following ovulation induction and intrauterine insemination: A case report. World Journal of Clinical Cases. 2021 Oct 16;9(29):8894. https://doi.org/10.12998/wjcc.v9.i29.8894
- Andrade AG, Rocha S, Marques CO, Simoes M, Martins I, Biscaia I, Barros CF. Ovarian ectopic pregnancy in adolescence. Clinical Case Reports. 2015 Sep 15;3(11):912. https://doi.org/10.1002/ccr3.336
- Aydin T, Yucel B, Aksoy H, Ekemen S. Successful laparoscopic management of a rare complication after embryo transfer: ovarian pregnancy. A case report and up-to-date literature review. Videosurgery and Other Miniinvasive Techniques. 2016 Jan;10(4):574-9.https://doi.org/10.5114/wiitm.2015.55893
- Samara N, Bentov Y. Case report of ectopic ovarian pregnancy following fresh embryo transfer. Clinical Medicine Insights: Reproductive Health. 2016 Jan;10:CMRH-S40593. https://doi.org/10.4137/cmrh.s40593
- Gebeh AK, Amoako AA, Joseph O, Banerjee A. Laparoscopic surgery for ovarian pregnancy using diathermy hook with conservation of ovary: a case report and literature review. Journal of clinical medicine. 2013 Oct 31;2(4):214-9.https://doi.org/10.3390/jcm2040214
- Pascal FK, El Hanna J, Arsalane A, Denakpo JL. Ovarian pregnancy following fresh embryo transfer: A case report and literature review. Case Reports in Women’s Health. 2025 Aug 19:e00744. https://doi.org/10.1016/j.crwh.2025.e0074
- Seo MR, Choi JS, Bae J, Lee WM, Eom JM, Lee E, Keum J. Preoperative diagnostic clues to ovarian pregnancy: retrospective chart review of women with ovarian and tubal pregnancy. Obstetrics & gynecology science. 2017 Sep 18;60(5):462.https://doi.org/10.5468/ogs.2017.60.5.462
- Solangon SA, Naftalin J, Jurkovic D. Ovarian ectopic pregnancy: clinical characteristics, ultrasound diagnosis and management. Ultrasound in Obstetrics & Gynecology. 2024 Jun;63(6):815-23.https://doi.org/10.1002/uog.27549
- Tanabe S, Suzuki T, Shiojima S, Nakayama S, Adachi H. Non-Tubal Ectopic Pregnancy. Journal of Clinical & Diagnostic Research. 2021 Sep 1;15(9). https://doi.org/10.7860/jcdr/2021/48986.15326
- Le AW, Wang ZH, Shan L, Dai XY, Xiao TH, Li XR. Clinical analysis of 95 cases with ovarian pregnancy. Clin. Exp. Obstet. Gynecol. 2016 Dec 10;43(6):2016.https://doi.org/10.12891/ceog3110.2016
- Kazal O, Ali AA. Ovarian pregnancy in a patient with a levonorgestrel intrauterine system in situ. International Journal of Gynecology & Obstetrics. 2012 Apr;117(1):82-3. https://doi.org/10.1016/j.ijgo.2011.11.006
- Qing X, Xie M, Zhang Y, Ma Y. Ruptured primary ovarian pregnancy: A case report with a literature review. Medicine. 2024 Jul 19;103(29):e39023. https://doi.org/10.1097/md.0000000000039023
- Alkatout I, Honemeyer U, Strauss A, Tinelli A, Malvasi A, Jonat W, Mettler L, Schollmeyer T. Clinical diagnosis and treatment of ectopic pregnancy. Obstetrical & gynecological survey. 2013 Aug 1;68(8):571-81. https://doi.org/10.1097/ogx.0b013e31829cdbeb
- Ren F, Liu G, Wang T, Li M, Guo Z. Unruptured ovarian ectopic pregnancy: Two case reports and literature review. Frontiers in Physiology. 2022 Oct 25;13:1036365. https://doi.org/10.3389/fphys.2022.1036365
- Ribeiro K, El Shamy T, Miskry T. Ovarian ectopic pregnancy after in vitro fertilisation treated by laparoscopic excision with ovarian preservation. BMJ Case Reports CP. 2020 Nov 1;13(11):e236680. https://doi.org/10.1136/bcr-2020-236680
- Kaur N, Reid F, Ma K. Ovarian ectopic pregnancy: laparoscopic excision and ovarian conservation. Journal of Minimally Invasive Gynecology. 2019 Sep 1;26(6):1006. https://doi.org/10.1016/j.jmig.2018.12.017
- Tambimuttu E, Lott A, Moore D. Successful diagnosis and laparoscopic management of haemorrhagic ovarian pregnancy with haemorrhagic contralateral corpus luteum. Australian & New Zealand Journal of Obstetrics & Gynaecology. 2015 Apr 1;55(2). https://doi.org/10.1111/ajo.12307
- Maree G, Mohammad S, Moualla Z, Alshoumary L, Makhos R, Alfarra A. Spontaneous ovarian and intrauterine non-viable heterotopic pregnancy at 12 weeks of gestation: a case report. Case Reports in Women’s Health. 2022 Jul 1;35:e00423. https://doi.org/10.1016/j.crwh.2022.e00423
- Hong YH, Kim H, Kim SK, Jee BC. A case of heterotopic ovarian pregnancy after in vitro fertilization: Early diagnosis and single-port access conservative laparoscopic treatment. Gynecology and Minimally Invasive Therapy. 2021 Jan 1;10(1):57-60. https://doi.org/10.4103/gmit.gmit_117_19
- Gundabattula SR, Resapu P, Surampudi K, Surapaneni T, De Padua M. Ovarian apoplexy resulting from ruptured heterotopic pregnancy following intrauterine insemination. Journal of Obstetrics and Gynaecology Research. 2017 Jul;43(7):1222-6. https://doi.org/10.1111/jog.13346
- Lee J, Kim KJ, Lee KM, Kim KA, Hong SK, Baek SK, Mun J, Bak S. Laparoscopic management of a bilateral ovarian pregnancy after failed methotrexate treatment. Clin. Exp. Obstet. Gynecol. 2017 Aug 10;44(4):2017. https://doi.org/10.12891/ceog3476.2017
- Eom JM, Choi JS, Bae J, Lee WM, Lee E, Lee J, Keum JH. Coexisting ovarian and tubal pregnancies on opposite sides after intrauterine insemination: a case report. BMC Pregnancy and Childbirth. 2018 Jun 25;18(1):259. https://doi.org/10.1186/s12884-018-1801-6
- Trindade VD, Burmann L, Viégas D, Hentschke MR, Azambuja R, Okada L, Petracco RG, Petracco A, Badalotti M, da Rosa Michelon J. Ectopic pregnancy in left ovary and contralateral uterine tube diagnosed one week apart in In Vitro Fertilization with donor eggs: Case report. JBRA Assisted Reproduction. 2019 Oct;23(4):439. https://doi.org/10.5935/1518-0557.20190030
- Huang Y, Huang Q, Liu J, Guo M, Liu Y, Lai D. Concurrent ovarian and tubal ectopic pregnancy after IVF-et: Case report and literature review. Frontiers in Physiology. 2022 Apr 4;13:850180. https://doi.org/10.3389/fphys.2022.850180
- Melcer Y, Smorgick N, Vaknin Z, Mendlovic S, Raziel A, Maymon R. Primary Ovarian Pregnancy: 43 Years Experience in a Single Institute and still a Medical Challenge. The Israel Medical Association Journal: IMAJ. 2015 Nov 1;17(11):687-90.
- Feit H, Leibovitz Z, Kerner R, Keidar R, Sagiv R. Ovarian pregnancy following in vitro fertilization in a woman after bilateral salpingectomy: a case report and review of the literature. Journal of Minimally Invasive Gynecology. 2015 May 1;22(4):675-7. https://doi.org/10.1016/j.jmig.2015.01.018
- Ota K, Takahashi T, Ota Y, Saito W, Nishimura H, Moriya T, Shimoya K. Pathogenesis and symptom of early hemorrhage in extrafollicular ovarian pregnancy onset at 4weeks gestation: A case report. International Journal of Surgery Case Reports. 2025 Jul 10:111647. https://doi.org/10.1016/j.ijscr.2025.111647
- Hirahara Y, Nagai K, Mukaida K. Live Births After Laparoscopic Wedge Resection for Unruptured Ovarian Pregnancy With Hemorrhagic Hypotension: A Case Report. Clinical Case Reports. 2025 Jan;13(1):e70044. https://doi.org/10.1002/ccr3.70044
- Ramalho I, Ferreira I, Marques JP, Carvalho MJ, Lobo A, Rebelo T, Moura JP, Águas F. Live birth after treatment of a spontaneous ovarian heterotopic pregnancy: A case report. Case Reports in Women’s Health. 2019 Oct 1;24:e00144. https://doi.org/10.1016/j.crwh.2019.e00144
- Tsubamoto H, Wakimoto Y, Wada R, Takeyama R, Ito Y, Harada K. Detection of unruptured ovarian pregnancy subsequently successfully treated by conservative laparoscopic surgery: a case report and review of the literature. Clinical and Experimental Obstetrics & Gynecology. 2013 Jan 1;40(4):604-6.
- Tabassum M, Atmuri K. The unexpected ovarian pregnancy at laparoscopy: a review of management. Case Reports in Obstetrics and Gynecology. 2017;2017(1):9856802. https://doi.org/10.1155/2017/9856802
- Ishikawa H, Sanada M, Shozu M. Ovarian pregnancy associated with a fresh blastocyst transfer following in vitro fertilization. Journal of Obstetrics and Gynaecology Research. 2015 Nov;41(11):1823-5. https://doi.org/10.1111/jog.12790
- Po L, Thomas J, Mills K, Zakhari A, Tulandi T, Shuman M, Page A. Guideline No. 414: management of pregnancy of unknown location and tubal and nontubal ectopic pregnancies. Journal of Obstetrics and Gynaecology Canada. 2021 May 1;43(5):614-30. https://doi.org/10.1016/j.jogc.2021.01.002
- Almahloul ZA, Amro BY, Nagshabandi ZK, Alkiumi IZ, Hakim ZT, Wattiez A, Tahlak MA, Koninckx PR. Ovarian Pregnancy: A Systematic Review and 2 Case Reports. https://doi.org/10.20944/preprints202212.0520.v1
- Alalade AO, Smith FJ, Kendall CE, Odejinmi F. Evidence-based management of non-tubal ectopic pregnancies. Journal of Obstetrics and Gynaecology. 2017 Nov 17;37(8):982-91. https://doi.org/10.1080/01443615.2017.1323852
- Stanley R, Nair A, Fiallo F. Spontaneous ovarian heterotopic pregnancy. Case Reports. 2018 Aug 9;2018:bcr-2018. https://doi.org/10.1136/bcr-2018-225619
- Dunphy L, Wood F, Hallchurch J, Douce G, Pinto S. Ruptured ovarian ectopic pregnancy presenting with an acute abdomen. BMJ Case Reports CP. 2022 Dec 1;15(12):e252499. https://doi.org/10.1136/bcr-2022-252499
- Hasegawa L, Nascu P, McNaught J. Ovarian ectopic pregnancy as IVF complication: first report in a gestational carrier. Case Reports in Obstetrics and Gynecology. 2018;2018(1):8190805. https://doi.org/10.1155/2018/8190805
- Obeidi N, Tchrakian N, Saadeh FA, Mocanu E. Suspected ovarian molar pregnancy after assisted reproductive technology conception: a diagnostic challenge. Case Reports. 2015 Apr 2;2015:bcr2015209353. https://doi.org/10.1136/bcr-2015-209353
- Sueldo C, Budinetz T, Maslow BS, Nulsen J, Engmann L, Benadiva C. Concurrent ovarian and ipsilateral tubal ectopic pregnancies after a double embryo transfer: a case report. Journal of assisted reproduction and genetics. 2014 Dec;31(12):1643-6. https://doi.org/10.1007/s10815-014-0338-5
- Deckers P, Ribeiro SC, Simões RD, da Fonseca Miyahara CB, Baracat EC. Systematic review and meta-analysis of the effect of bipolar electrocoagulation during laparoscopic ovarian endometrioma stripping on ovarian reserve. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2018 Jan;140(1):11-7. https://doi.org/10.1002/ijgo.12338
- Pergialiotis V, Prodromidou A, Frountzas M, Bitos K, Perrea D, Doumouchtsis SK. The effect of bipolar electrocoagulation during ovarian cystectomy on ovarian reserve: a systematic review. American journal of obstetrics and gynecology. 2015 Nov 1;213(5):620-8. https://doi.org/10.1016/j.ajog.2015.04.006
- Mohamed ML, Nouh AA, El-Behery MM, Mansour SA. Effect on ovarian reserve of laparoscopic bipolar electrocoagulation versus laparotomic hemostatic sutures during unilateral ovarian cystectomy. International Journal of Gynecology & Obstetrics. 2011 Jul 1;114(1):69-72. https://doi.org/10.1016/j.ijgo.2011.01.010