Case Report
HJOG 2026, 25 (3), 286-292 | doi: 10.33574/hjog.0636
Konstantinos Louis1, Spyridon Topis1, Anastasios Potiris1, Chrysi Christodoulaki2, Dimos Sioutis1, Anna Koumarianou3, Peter Drakakis1, Periklis Panagopoulos1, Sofoklis Stavros1
1Third Department of Obstetrics and Gynecology, “Attikon” University General Hospital, National and Kapodistrian University of Athens, Athens, Greece
2Department of Obstetrics and Gynecology, General Hospital of Chania “Agios Georgios”, Chania, Greece
3Oncology Unit, Fourth Department of Internal Medicine, “Attikon” University General Hospital, National and Kapodistrian University of Athens, Athens, Greece
Correspondence: Konstantinos Louis, Third Department of Obstetrics and Gynecology, “Attikon” University General Hospital, National and Kapodistrian University of Athens, Athens, Greece, Tel.: +30 2105832244, e-mail: kostaslouisss@gmail.com
![]()
Abstract
Introduction: Pregnancy associated breast cancer (PABC) is a rare yet important clinical presentation that generally refers to breast cancer diagnosed during pregnancy, lactation or within the year following delivery. It represents the most frequent cancer detected during pregnancy, even though it is rare, with prevalence of approximately 1 per 3,000 pregnancies, and recent meta-analytical data has placed its incidence at 19.2 per 100,000 pregnancies worldwide. Breast physiology during pregnancy and lactation impacts on diagnosis and on delayed presentation of a more advanced disease.
Materials and Methods: We describe a case of a 35-year-old woman presented at 14 weeks of pregnancy following identification of a lump in the right breast during self-palpation. Following assessment, the patient had a mammography, breast ultrasound and core needle biopsy with histopathology and immuno-histochemistry assessment. Maternal-fetal monitoring was instituted, and a multidisciplinary tumor board consultation was held.
Results: A mammography reported BI-RADS V, while an ultrasound confirmed a suspicious lesion in the right breast with suspicious involvement of the right axilla. Histopathology revealed an invasive carcinoma of no special type (NST) with Nottingham grade 2, the tumor showed ER expression of 60%, PR expression of 20% and Ki 67 expression of 20%. Paclitaxel was administered during the pregnancy following multidisciplinary team decision. No fetal or maternal complications occurred during pregnancy. At 36 weeks of gestation, a live male neonate weighing 2830 g was delivered. Subsequent postpartum staging revealed distant hepatic metastasis and treatment with systemic therapy resulted in significant disease regression.
Conclusions: This case highlights the importance of not attributing every palpable breast mass detected during pregnancy to physiological gestational changes, early investigation, appropriate multidisciplinary management and tailored treatment protocols are crucial in pregnancy associated breast cancer for the best outcome for both mother and infant.
Key words: Pregnancy-associated breast cancer, breast cancer, pregnancy, paclitaxel, maternal-fetal medicine, multidisciplinary management
Introduction
PABC stands for pregnancy-associated breast cancer, and defines as the breast cancer diagnosed during pregnancy, during lactation, or during the first year postpartum1. The physiological changes of the breast during pregnancy involve hyperplasia and glandular hyperplasia, which are increases in gland tissue volume, and are accompanied by increased vascularization and gland density. While this transformation is normal in anticipation of lactational activity, it can also be confusing, thereby masking disease or resulting in the delay of a definitive diagnosis of suspicious breast lesion1,4. In the pregnant patient who has been diagnosed with cancer, there are two unrelated clinical entities that must be integrated into a complex system, in which maternal care and fetal welfare are intertwined.
Pregnancy-associated breast cancer (PABC) is breast cancer diagnosed during pregnancy, while lactating, or while within one year of delivery1. Although rare, the clinical significance of PABC has grown in recent years. Changes in reproductive behaviour such as childbearing deferral in developed countries mean that a larger percentage of pregnancies now occur during a woman’s lifetime risk period for developing breast cancer2,3, and therefore maternal health care providers may be more likely to see such cases in their daily practice.
One of the biggest challenges with PABC is prompt diagnosis. Physiological changes in the breasts during pregnancy include glandular proliferation and hyperplasia, an increase in gland tissue volume, increased vascularization and gland density. Although these changes are to be expected to prepare the breasts for lactation, they are also a source of interference that may disguise pathological processes or cause a physician to delay a definitive diagnosis of suspicious breast lesion1,4.
As a consequence of delayed diagnosis, the patient with PABC will often present with more large masses and have a higher rate of nodal metastasis and more advanced disease than similar-aged patients who are not pregnant3,6. These facts have prompted researchers to try to determine if the outcome difference for the PABC patient is due to the delay in diagnosis or if there may be an alteration in tumor biology itself due to pregnancy.
In addition to its clinical and diagnostic challenges, PABC poses significant psychosocial burdens. While pregnancy often represents a time of excitement and positive expectation focused on welcoming new life into the world, the concurrent diagnosis of a life-threatening illness can cause deep psychological disturbances. Patients are faced with distressing choices relating to treatment commencement, the potential harm to their fetus, maintaining the pregnancy, breastfeeding, and the patient’s long-term survival, and are not surprisingly associated with a significantly high degree of psychological morbidity1,11. The biological factors underlying PABC have not been well studied, though developments in the molecular characterization of breast cancer as a whole are providing insight into a more biologically distinct profile in pregnancy-associated malignancies that may be influenced by the hormonal and immunological milieu of the pregnant state, leading to differential tumor biology and potentially influencing therapeutic strategies8,9. We present a case of a second-trimester breast cancer in pregnancy, and review the current literature on diagnosis, therapeutic strategies, maternal-fetal monitoring and the benefit of a multidisciplinary approach.
Case Presentation
A 35-year-old G3 P2 woman with a history of 2 previous CS presented at 14 weeks gestation having discovered a palpable mass in her right breast during self-examination while being weaned from breast-feeding. She reported no breast pain, discharge, or any constitutional signs/symptoms.
On clinical examination she had a firm palpable lesion in her right breast. Subsequent work up was performed. Mammography was performed using appropriate fetal shielding and was classified as BI-RADS V. Breast ultrasound revealed a suspicious solid mass with features concerning for malignancy, along with suspicious axillary nodes (Figures 1 and 2). She underwent an ultrasound-guided core biopsy at 15 weeks and 5 days gestation. Histopathological assessment confirmed an invasive breast carcinoma of no special type, Nottingham grade 2. Hormone receptor testing revealed a positive ER in 60%, a positive PR in 20% and Ki67 expression of 20%. Due to the pregnancy being ongoing staging workup was initially deferred. CA 15-3 levels were found to be raised at 108 U/mL. A non-contrast MRI scan of thorax and abdomen was performed, which revealed suspected bone lesions concerning metastatic diseases.
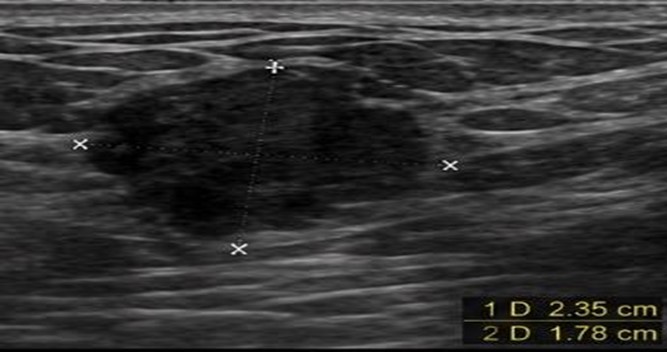
Figure 1. Grayscale ultrasonography showing an irregular solid mass with non – circumscribed margins and heterogeneous internal echotexture,measuring 2.35cm x 1,78cm.
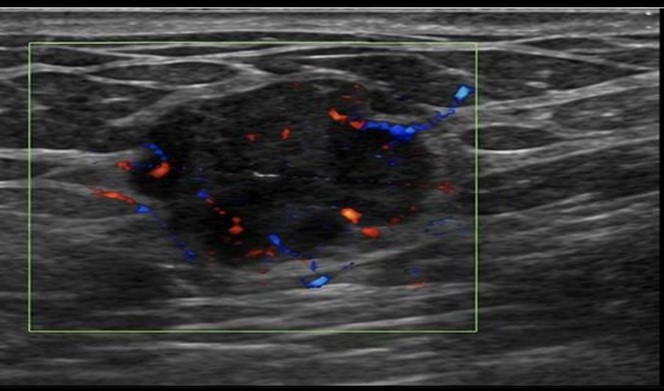
Figure 2. Colour Doppler ultrasonography of the same lesion demonstrating increased internal and peripheral vascularity, findings suggestive of neoplastic angiogenesis.
After discussion within a multidisciplinary team (MDT) comprising maternal–fetal medicine specialists, oncologists, breast surgeons, radiologists, and neonatologists, the decision was made to initiate 12 cycles of chemotherapy with paclitaxel until delivery, taking into consideration the gestational age, tumor biology and extent of disease, as well as fetal safety. The patient responded well to chemotherapy and tolerated treatment without significant complications (Figure 3).
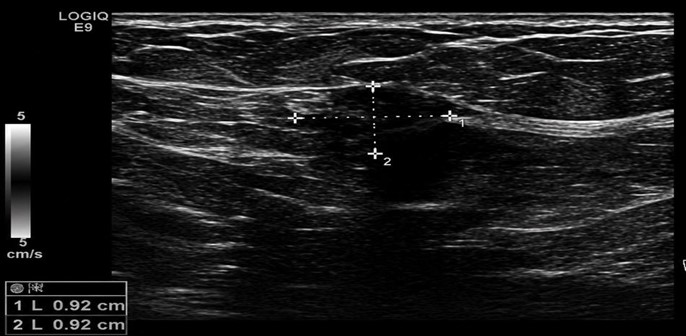
Figure 3. Breast Ultrasonography after the first six cycles of paclitaxel shows smaller mass with measuring 0,92cm x 0,92cm.
Fetal surveillance was performed with serial ultrasound assessments of growth and Doppler studies, which remained within normal limits throughout pregnancy. The patient also underwent cardiac evaluation to monitor for potential chemotherapy-related cardiotoxicity, with no abnormalities detected. She delivered a male infant at 36 weeks’ gestation, weighing 2,830gr, with no abnormalities identified on neonatal assessment.
Following delivery, the patient’s staging workup was completed and revealed liver metastases. She subsequently commenced further oncological treatment. Follow-up imaging demonstrated a favorable response, with markedly reduced uptake in the metastatic lesions, although small residual liver lesions remained detectable.
The chronological sequence of clinical events is presented in Table 1.
Discussion
Diagnostic challenges of pregnancy-associated breast cancer
Pregnancy-associated breast cancer (PABC) continues to be one of the most difficult clinical challenges facing modern medicine. Physiological changes to the breast during pregnancy, including hyperplasia and hypertrophy of glandular tissue, enhanced vascularity, edema, and nodularity, may make clinical examination more difficult and obscure subtle abnormalities1,4. Consequently, malignant lesions can be initially confused with the more typical changes of gestation, and there is delayed diagnosis.
This diagnostic difficulty has important clinical implications. Women with PABC often present with larger lesions, greater axillary involvement and higher stage disease than matched non-pregnant breast cancer patients3,6. It is still unclear whether this is due to an intrinsically more aggressive biology, or simply delayed diagnosis.
Our patient was alerted to a lump through breast self-examination, an informal rather than formal screening method, and it seems appropriate to counsel pregnant women to be aware of persistent or concerning breast changes. Clinicians should also have a low index of suspicion for abnormalities of the breast during pregnancy and act on such concerns especially if they persist or demonstrate concerning features4.
Imaging and staging in pregnancy
Fear of harm to the fetus often impacts on choices about imaging. However, breast ultrasonography should be seen as safe and is highly sensitive in evaluating breast masses in pregnancy1,4. Mammography is also considered safe in pregnancy with adequate shielding as fetal radiation is minimized.
Histological diagnosis is critical and should not be delayed as many treatment decisions are dependent upon receptor status, proliferative indices and pathology4. Many of the standard staging procedures for breast cancer need adaptation during pregnancy. MRI without gadolinium may provide useful information in some patients and is often utilized to look for distant metastatic disease. In the case reported here, possible bony metastatic deposits were visualized by MRI in pregnancy, while postpartum staging confirmed hepatic metastases. This represents a common dilemma in the management of PABC, balancing the need for appropriate oncological assessment with minimization of fetal risk.
Epidemiological data
Though rare PABC seems to be an increasing incidence worldwide. Delayed childbearing has become one of the major causes and increased number of women are conceiving in age groups with increased basal risk of breast cancer2,3. A recent systematic review and meta-analysis revealed global incidence as about 19.2 cases/100,000 pregnancies2 Thus, clinicians involved in obstetric practice may face PABC in an increasing frequency. Furthermore, changing reproductive trends, including increased utilization of assisted reproductive technologies continue to generate questions regarding the relationship between hormones and cancer. While no causal link has been proven, more longitudinal studies in this area are required.
Biological behaviour and molecular types
The biology of PABC is poorly understood. Pregnancy is a state associated with profound changes in hormonal balance, an increase in the growth factors, such as estro gens and progesterone, increased angiogenesis and appropriate immune adaptation required for maintenance of pregnancy8,9.
Several authors hypothesize that these changes may promote the growth and metastatic potential of breast cancer8,9. Postpartum breast involution has also been linked to inflammatory and remodelling pathways which might promote tumor aggressiveness8. A study by Suelmann et al. revealed differences in clinicopathological features depending on gestational timing of diagnosis, indicating that disease diagnosed during pregnancy and lactation might not be a homogenous entity6. Recent molecular studies revealed that changes occur within the pathways involving inflammation, angiogenesis, cell proliferation, and immune regulation9. It is yet unknown whether pregnancy inherently worsens prognosis, or whether the poor prognosis is due to a longer latency to diagnosis with subsequent advanced stage disease.
In our patient ER/PR positivity led to important therapeutic decisions, namely adjuvant endocrine treatment post-delivery. Ki-67 revealed moderately increased proliferation. However, the subsequent metastases demonstrated the significant prognostic impact of stage at diagnosis.
Psychological burden and patient-centered care
Psychological impact of having cancer during pregnancy is significant and should never be overlooked. Women are forced to cope with the implications of their diagnosis for their own survival and future, as well as the safety of their unborn child and the potential harm posed by treatment7. Clinically patients are more often worried about the safety of their fetus than their own future prognosis. Most decisions are made in a state of emotional overwhelming and under extremely strict time limits. Therefore, treatment should not just be oncologically focused. Psychological and family-centered care needs to be an integral part of management1,11.
Multidisciplinary management and treatment
Our case further highlights the value of multidisciplinary collaboration in management of PABC. These women have conflicting demands that need to be addressed, including mother’s need for effective treatment, the safety of the fetus, and the requirements of obstetric practice.
It is now clear, according to ESMO guidelines, that treatment cannot be approached as it would be for non-pregnant women and should involve multiple specialists4. Our patient’s treatment plan, like those of many other PABC cases, was shaped by multidisciplinary input and decision making. This individualized approach will continue to play a central role. Chemotherapy initiated after first trimester appears safe for mother and fetus4,10. Increasing data regarding taxanes indicate that paclitaxel may be a safe and effective therapeutic option in carefully selected patients5.
The favorable fetal outcome in our case suggests that systemic therapy administered later in pregnancy may be feasible when accompanied by vigilant maternal and fetal monitoring.
Long-term outcomes
Both mother and child need long-term follow-up. Present data does not suggest that prenatal exposure to chemotherapy after first trimester significantly impact neurological and cardiac outcome; however future follow-up remains essential10.
However, despite all advances, knowledge on PABC still needs significant improvement. Being a rare condition, collaborative studies involving numerous centers worldwide are necessary to improve understanding of PABC and treatment strategies9,11.
Conclusions
Pregnancy-associated breast cancer (PABC) represents a clinically challenging condition that requires timely recognition and individualized management. Pregnancy should not lead to postponement of the evaluation of suspicious breast findings. This case highlights the importance of early diagnosis, prompt therapeutic planning, and multidisciplinary collaboration. It also supports the existing evidence suggesting that systemic treatment after the first trimester can be administered with an acceptable fetomaternal safety profile in carefully selected cases. Optimal management depends on close cooperation among specialties and a careful balance between maternal benefit and fetal safety. Further studies and international collaboration are needed to refine treatment strategies and improve outcomes for women diagnosed with PABC.
Disclosure
The authors report no conflict of interest
Ethics Statement
The study was conducted in accordance with the World Medical Association Declaration of Helsinki. The patient has given her written informed consent to publish the case (including the publication of images obtained).
Consent
Written informed consent was obtained from the patient to publish this report in accordance with the journal’s patient consent policy.
Funding
None to disclose for all authors.
References
- Galati F, Magri V, Arias-Cadena PA, et al. Pregnancy-associated breast cancer: a diagnostic and therapeutic challenge. Diagnostics (Basel). 2023;13(4):604. doi:10.3390/diagnostics13040604.
- Akhlaqi M, Ghofrani A, Najdi N, et al. A systematic review and meta-analysis of pregnancy-associated breast cancer incidence rate. BMC Cancer. 2025;25:660. doi:10.1186/s12885-025-14091-2.
- Tan QT, Alcantara VS, Sultana R, et al. Pregnancy-associated breast cancer: a multicenter study comparing clinicopathological factors, diagnosis and treatment outcomes with non-pregnant patients. Breast Cancer Res Treat. 2023;198(1):53–66.
- Loibl S, Azim HA Jr, Bachelot T, et al. ESMO Expert Consensus Statements on the management of breast cancer during pregnancy. Ann Oncol. 2023;34(10):849–866.
- Girardelli S, Lambertini M, et al. Weekly paclitaxel for pregnancy-associated breast cancer. Clin Breast Cancer. 2024.
- Suelmann BBM, van Dooijeweert C, Bakhuis CFJ, et al. Pregnancy-associated breast cancer: the influence of gestational age. Endocr Relat Cancer. 2022;29(3):129–138.
- Amant F, Vandenbroucke T, Verheecke M, et al. Pediatric outcome after maternal cancer diagnosed during pregnancy. N Engl J Med. 2015;373:1824–1834.
- Sajjadi E, Venetis K, et al. Immune microenvironment dynamics in breast cancer during pregnancy and lactation. Eur J Cancer Prev. 2023.
- Peña-Enríquez R, et al. Molecular characterization of pregnancy-associated breast cancer. NPJ Breast Cancer. 2025.
- Huis in ’t Veld EA, et al. Long-term outcomes of children after prenatal exposure to maternal cancer and its treatment. Acta Obstet Gynecol Scand. 2024;103:757–760.
- Roesch E, et al. Pregnancy-associated breast cancer: key concepts for optimizing care. JCO Oncol Pract. 2024.