Review
HJOG 2026, 25 (3), 198-207 | doi: 10.33574/hjog.0628
Donel Suhaimi, Renardy Reza Razali, Sofyan Andri, Kalvin Tutamana Hutabarat
Department of Obstetrics and Gynecology, Faculty of Medicine Riau University, Pekanbaru, Indonesia
Correspondence: Donel Suhaimi, Jl. Ismail Yusuf RT 006/RW 002, Tangkerang Tengah, Marpoyan Damai, Pekanbaru, Riau, Tel./Fax: 0811660685, e-mail address: donel@lecturer.unri.ac.id
![]()
Abstract
Background: Air travel during pregnancy has become increasingly common in line with the rising mobility of women of reproductive age. Although generally considered safe for uncomplicated pregnancies, potential risks may vary across different trimesters.
Objective: To evaluate trimester-specific health risks associated with air travel in pregnant women by reviewing evidence from observational studies.
Methods: This systematic review was conducted following PRISMA guidelines. Literature searches were performed in PubMed, Google Scholar, EuropePMC, and ScienceDirect from June 2015 to June 2025 using keywords “air travel,” “pregnancy,” “trimester,” and “maternal or fetal outcomes.” Eligible studies were observational in design (cohort, case-control, or cross-sectional) and reported the impact of air travel according to pregnancy trimester.
Results: Seven studies met the inclusion criteria. First-trimester air travel was associated with an increased risk of early miscarriage, particularly among women undertaking flights ≥15 hours with irregular sleep schedules. The second trimester was identified as the safest period, with the lowest risk of complications. Air travel in the third trimester was generally considered safe, even for high-risk pregnancies, provided thorough preparation and adherence to medical recommendations were ensured. Nonetheless, caution remains warranted due to potential risks such as venous thromboembolism (VTE), reduced cabin oxygen levels, and delayed access to medical care during emergencies.
Conclusion: The risks of air travel during pregnancy vary by trimester. The second trimester appears to be the safest period, while additional vigilance is required for first- and third-trimester travel. Individual clinical assessment remains essential before granting medical clearance for pregnant women to fly.
Key words: Pregnancy, air travel, trimester, maternal risks, pregnancy outcomes
Introduction
Air travel is one of the most widely used methods of transportation by people around the world, including pregnant women. In recent decades, the increasing involvement of women in professional and social activities has led to more pregnant women taking domestic and international flights. This situation has prompted the need for a deeper understanding of the safety of air travel during pregnancy.1
Pregnancy is a complex physiological condition, characterized by various adaptive changes in the cardiovascular, respiratory, hematological, and metabolic systems. These factors can be exacerbated by conditions in the aircraft cabin, such as lower air pressure, low humidity, prolonged immobilization, and limited access to medical services during flight. Therefore, there are concerns that air travel may affect the health of both the mother and the fetus, especially in pregnancies with certain medical conditions or at certain gestational ages.2
Guidelines from various professional organizations, including the American College of Obstetricians and Gynecologists (ACOG) and the Royal College of Obstetricians and Gynaecologists (RCOG), generally state that air travel is safe for uncomplicated pregnancies. However, these guidelines are still general in nature and do not explicitly differentiate risks based on the trimester of pregnancy. This poses a challenge in clinical practice, given that each trimester has different physiological characteristics and potential complications, such as the risk of miscarriage in the first trimester or premature labor in the third trimester.1
The first, second, and third trimesters of pregnancy show different biological changes, both in the mother and the fetus. Therefore, the risks that may arise from exposure to flight conditions also vary according to the stage of pregnancy. This can make it difficult to make appropriate and evidence-based clinical decisions, especially when counseling pregnant women who are planning to travel by air.3
This systematic review was conducted to evaluate the risks of air travel for pregnant women specifically based on the trimester of pregnancy, using evidence from observational studies. This study is expected to be a useful scientific contribution in strengthening clinical practice guidelines and maternal health policies, as well as providing a more appropriate basis for consideration in providing air travel recommendations to pregnant patients.
Methods
This research method was designed as a systematic review based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines as shown in Figure 1. Literature was systematically searched in four major electronic databases, namely PubMed, Google Scholar, EuropePMC, and ScienceDirect, for publications published between June 2015 and June 2025. The search strategy used a combination of Medical Subject Headings (MeSH) and related keywords, including the terms “pregnancy,” “pregnant women,” “air travel,” “flying,” “flight,” “trimester,” and ‘maternal’ and “fetal outcomes.” Studies that met the inclusion criteria were observational studies (prospective or retrospective cohorts, case-control, and cross-sectional) involving pregnant women at various stages of pregnancy who traveled by commercial air and reported maternal and fetal risk outcomes such as preterm birth, venous thromboembolism, miscarriage, fetal growth restriction, or other obstetric complications. Only full-text articles published in English or Indonesian within the last 10 years were included. Randomized controlled trials (RCTs), narrative reviews, editorials, letters to the editor, and studies on non-human populations or non-commercial flights were excluded. The study selection process was conducted independently by two researchers, with data extracted including author names, year of publication, study design, number of participants, trimester of pregnancy, type of outcome, and main results. Study quality was assessed using the Newcastle-Ottawa Scale for cohort and case-control studies, and the AXIS tool for cross-sectional studies, to ensure the validity and reliability of the synthesized findings.
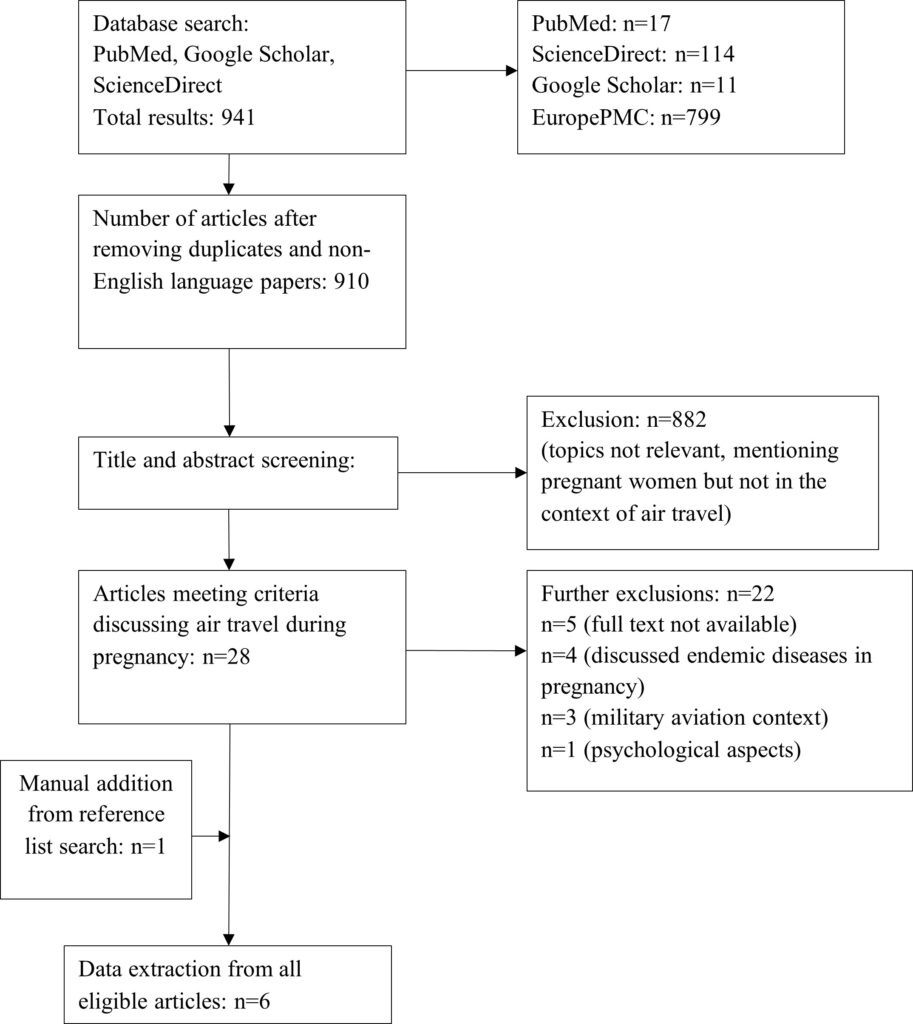
Figure 1. PRISMA flowchart for literature research.
Result
The systematic search yielded a total of 941 search results, and after removing duplicates and articles in foreign languages, 910 articles remained. During the title and abstract screening process, we selected 28 articles for in-depth review. During the in-depth review process, we excluded 22 articles for the following reasons: 9 articles were reviews of existing guidelines and research.1,4–11, 5 articles are not available in full text.12–16, 4 studies mentioned about infection in endemic areas through air travel8,17–19, 3 articles reported about pregnancy in military air travel20–22, and one study mentioned about the psychological aspect of pregnant women regarding air travel23. In addition, we also conducted additional searches by reviewing the references of 28 articles that were included in the systematic search and related review articles, and found 1 additional article.24. A total of 6 observational studies were eligible for inclusion in this systematic review.24–29
This review covers six observational studies published between 2015 and 2024 that met the established inclusion criteria. Of these studies, five were retrospective cohorts and one was a cross-sectional study, with the number of participants ranging from 16 to more than 600,000 individuals. The studies originated from various countries and assessed a range of pregnancy-related outcomes associated with air travel, including miscarriage, venous thromboembolism (VTE), preterm birth, birth weight, fetal movement, and complications in multiple pregnancies with Twin-to-Twin Transfusion Syndrome (TTTS). The detailed findings are explained in Table 1.
The analysis was further divided by pregnancy trimester to explore how the timing of exposure and maternal conditions might influence outcomes. By categorizing women in their first, second, and third trimesters, we were able to see differences in vulnerability and potential variations of effect in air travel.
- First Trimester
Two studies examined the risks of air travel during the first trimester. Grajewski et al. found an increased risk of miscarriage among flight attendants who flew ≥15 hours during local nighttime hours. Heidecker et al. reported a higher incidence of miscarriage among flight attendants than in the general population, but this was not associated with exposure to second-hand smoke.
- Second Trimester
A study with a big population by Ram et al. showed that air travel during the second trimester was associated with a statistically significant, but not clinically significant, increase in gestational age and birth weight. This supports the notion that the second trimester is a relatively safe period for flying.
- Third Trimester
Two studies evaluated risks in the third trimester. Petrikovsky et al. reported changes in fetal movement during and after flight, but showed no long-term effects. Tchirikov et al. assessed the safety of long-distance medical air travel for TTTS patients and concluded that air transport is safe if properly prepared.
- Trimester Not Specified
One study by Ram et al. (2023) did not specify a particular trimester, but reported a statistically significant increase in the risk of venous thromboembolism after flying, even though the absolute incidence was low. This highlights the importance of paying attention to the risk of VTE in pregnant women who travel by plane.
Discussion
This systematic review evaluates the risks of air travel in pregnant women based on the trimester of pregnancy, using data from six observational studies published between 2015 and 2024. The results of this review indicate that air travel during pregnancy has a varying risk profile depending on the gestational age at exposure, with the second trimester generally considered the safest, while the first and third trimesters show certain potential risks, although the evidence is still limited and heterogeneous.
Risks in the First Trimester
Studies evaluating air travel during the first trimester report an increased risk of miscarriage, particularly in women with high exposure duration or in occupations involving shift work.26 Grajewski et al. (2015) found that exposure to ≥15 hours of flight time during local nighttime sleep was associated with an increased risk of miscarriage (RR 1.5; 95% CI 1.1–2.2). This study highlights the importance of considering circadian aspects in early pregnancy flight safety. Another study by Heidecker et al. (2017) noted a higher incidence of miscarriage among flight attendants, although it was not statistically proven to be associated with exposure to secondhand smoke.29
These findings are consistent with previous literature showing that the first trimester is a critical phase in embryonic development, with susceptibility to implantation disorders, physiological stress, and hormonal changes, making pregnant women with irregular sleep patterns and heavy workloads more prone to miscarriage.30
Meanwhile, passengers on regular flights during the first trimester did not show a significant increase in miscarriage rates. There is no consistent evidence that regular passengers experience miscarriages as a result of occasional flights during the first trimester, especially in uncomplicated pregnancies.31,32 Therefore, air travel during the first trimester on short-haul flights without complications tends to be safe, but long-haul flights or irregular flights should be considered carefully.
Risks in the Second Trimester
A large study by Ram et al. (2020) involving more than 41,000 participants found that air travel during the second trimester was not associated with a clinically significant increase in the risk of obstetric complications.27 This study even reported a statistically significant, albeit small, increase in the average gestational age and birth weight.
These findings support recommendations long held by various professional organizations, including the American College of Obstetricians and Gynecologists (ACOG), which states that the second trimester is the safest period for air travel, as the risk of miscarriage has decreased, the nausea and vomiting of early pregnancy have passed, and the size of the uterus has not yet caused excessive discomfort.1,33,34
Risks in the Third Trimester
In the third trimester, two studies showed relatively convincing results. A study by Petrikovsky et al. noted temporary changes in fetal movement during transatlantic flights, but no long-term effects on the fetus.25 Meanwhile, Tchirikov et al. evaluated the safety of air travel in patients with twin-to-twin transfusion syndrome (TTTS) undergoing fetoscopic procedures and found no increased maternal or neonatal risk compared to ground transportation.24
These findings suggest that with proper medical preparation, even high-risk pregnancies can be safely transported by air.
However, air travel during the third trimester still needs to be approached with caution due to physiological risks such as inferior vena cava compression, increased risk of thromboembolism, and the possibility of spontaneous labor.3,35 This is also in line with the general restrictions imposed by airlines, which often limit flights after 36 weeks of pregnancy.2
Risk of Thrombosis and Other Non-Trimester-Specific Outcomes
A study by Ram et al. (2023), which did not specify the trimester, found an increased risk of venous thromboembolism (VTE) after air travel, with a hazard ratio of 1.406.28 Although the absolute incidence is low, this highlights the importance of preventive measures such as wearing compression stockings, staying hydrated, and moving around during flights — especially for pregnant women with additional risk factors such as obesity, a history of thrombosis, or multiple pregnancies.4
Strengths and Limitations of the Review
The strength of this review lies in its specific focus on trimesters, which are rarely discussed in previous literature, as well as its use of observational studies that reflect real-world clinical practice.
However, there are several limitations. First, the number of studies that met the inclusion criteria was relatively small, and most were retrospective in design. Second, the variability of outcomes, measurement methods, and heterogeneous population groups made quantitative synthesis (meta-analysis) impossible. Third, some studies used specific populations (e.g., flight attendants or referral patients with TTTS) that may not be generalizable to all pregnant women.
Conclusion
This systematic review shows that air travel during pregnancy has a varying risk profile depending on the trimester of pregnancy. The second trimester consistently emerges as the period with the lowest risk and is considered safe for pregnant women who have no medical complications. Conversely, the first trimester is associated with an increased risk of miscarriage, especially in cases of long flights or jobs with irregular working hours, so pregnant women in this situation need special attention. In the third trimester, although some studies indicate relative safety, potential risks such as premature labor, venous thromboembolism, and physical discomfort should still be considered, especially on long-haul flights.
Overall, air travel can be considered safe for most pregnant women, provided that individual clinical evaluation is still necessary before traveling, especially for groups with specific obstetric or medical risk factors. Air travel recommendations should consider the gestational age, flight duration, health status of the mother and fetus, and appropriate preventive measures such as mobilization, hydration, and the use of elastic compression.
Further research with prospective designs and more in-depth trimester-specific risk analyses is still needed to strengthen the evidence base and guide more specific clinical recommendations.
Conflict of Interest
The authors declare that there is no conflict of interest in the making of this article.
Acknowledgement
The authors would like to express their sincere gratitude to the staff of the Department of Obstetrics and Gynecology, Universitas Riau, for their continuous support, valuable guidance, and professional contribution throughout the preparation of this manuscript. Their academic input and institutional support have been instrumental in the successful completion of this work.
References
- Air Travel During Pregnancy [Internet]. 2018. Available from: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2018/08/air-travel-during-pregnancy
- Air Travel and Pregnancy (Scientific Impact Paper No. 1) | RCOG [Internet]. Air Travel and Pregnancy (Scientific Impact Paper No. 1) | RCOG; 2019. Available from: https://www.rcog.org.uk/guidance/browse-all-guidance/scientific-impact-papers/air-travel-and-pregnancy-scientific-impact-paper-no-1/
- Savona-Ventura C, Mahmood T. Commercial Air And High-Altitude Travel by Pregnant Women: A scientific review commissioned by the European Board and College of Obstetrics and Gynaecology (EBCOG). Eur J Obstet Gynecol Reprod Biol [Internet]. 2022 Jul;272:217–9. Available from: https://pubmed.ncbi.nlm.nih.gov/35381544/
- Csorba R, Tsikouras P, Bothou A, Zervoudis S, Iatrakis G, Anthoulaki X, et al. Air travel during pregnancy: An update review and practical recommendation. Clin Exp Obstet Gynecol [Internet]. 2019 Dec 1 [cited 2025 Jul 9];46(6):862–6. Available from: https://www.imrpress.com/journal/CEOG/46/6/10.12891/ceog4885.2019
- Cardona-Ospina JA, Salazar-Vargas CE, Barreto-Moreno JJ, Muñoz-Gaviria S, García-Sánchez T, Rodríguez-Morales AJ. Flying and pregnant? – Regulations of the main airlines in Latin America. Travel Med Infect Dis [Internet]. 2015 Jul 1 [cited 2025 Jul 6];13(4):335–7. Available from: https://www.sciencedirect.com/science/article/pii/S1477893915001155
- Jasper B, Aiken C. International travel during pregnancy: a review of current literature and guidelines. Obstet Gynaecol Reprod Med [Internet]. 2024 Dec 1 [cited 2025 Jul 6];34(12):338–43. Available from: https://www.sciencedirect.com/science/article/pii/S1751721424001416
- Savona-Ventura C, Mahmood T. A scientific review commissioned by the European board and college of obstetrics and gynaecology (EBCOG). European Journal of Obstetrics and Gynecology and Reproductive Biology [Internet]. 2022 May 1 [cited 2025 Jul 5];272:217–9. Available from: https://pubmed.ncbi.nlm.nih.gov/35381544/
- Hale GL. Flaviviruses and the Traveler: Around the World and to Your Stage. A Review of West Nile, Yellow Fever, Dengue, and Zika Viruses for the Practicing Pathologist. Modern Pathology [Internet]. 2023 Jun 1 [cited 2025 Jul 6];36(6). Available from: https://www.sciencedirect.com/science/article/pii/S0893395223000935
- Management CBP, 2017 undefined. Travel consultations: Pregnant travellers. magonlinelibrary.com [Internet]. 2017 May 2 [cited 2025 Jul 6];27(5):26–9. Available from: https://www.magonlinelibrary.com/doi/full/10.12968/prma.2017.27.5.26
- Mackell SM, Borwein S. The pregnant and breastfeeding traveler. Travel Medicine [Internet]. 2018 Jan 1 [cited 2025 Jul 6];225–36. Available from: https://www.sciencedirect.com/science/article/pii/B9780323546966000227
- Izadi M. Do pregnant women have a higher risk for venous thromboembolism following air travel? journals.lww.com [Internet]. [cited 2025 Jul 6]; Available from: https://journals.lww.com/adbm/fulltext/2015/04000/do_pregnant_women_have_a_higher_risk_for_venous.60.aspx
- Leung DT, LaRocque RC, Ryan ET. Travel medicine. acpjournals.org [Internet]. 2018 Jan 2 [cited 2025 Jul 6];168(1):ITC1–15. Available from: https://www.acpjournals.org/doi/abs/10.7326/AITC201801020
- Hurd W, Rothenberg J. Aeromedical evacuation of obstetric and gynecological patients. Springer [Internet]. 2019 [cited 2025 Jul 6];337–62. Available from: https://link.springer.com/chapter/10.1007/978-3-030-15903-0_21
- Sutherland S, Practical ROIFMEA, 2018 undefined. Preflight Therapies to Minimize Medical Risk Associated with Commercial Air Travel. Springer [Internet]. 2018 [cited 2025 Jul 6];141–9. Available from: https://link.springer.com/chapter/10.1007/978-3-319-74234-2_14
- McAlester C, Cesario S, health TKN for women’s, 2020 undefined. Travel health implications for women traveling abroad. Elsevier [Internet]. [cited 2025 Jul 6]; Available from: https://www.sciencedirect.com/science/article/pii/S1751485120300362
- Torresi J, McGuinness S, Leder K, O’Brien D, Ruff T, Starr M, et al. Travellers with special needs. Springer [Internet]. 2019 [cited 2025 Jul 6];297–376. Available from: https://link.springer.com/chapter/10.1007/978-981-13-7252-0_7
- Sharma KS, Sharma R, Nehra S, Rajpurohit NA, Bhakar K, Kumar D. COVID-19: Consequences on pregnant women and neonates. Health Sciences Review [Internet]. 2022 Sep [cited 2025 Jul 6];4:100044. Available from: https://www.sciencedirect.com/science/article/pii/S2772632022000332
- Curcio E, Baum J. Travel in Pregnancy: The Impact of Zika. scirp.org [Internet]. 2017 [cited 2025 Jul 6];7:1064–71. Available from: https://www.scirp.org/journal/paperinformation?paperid=79640
- Mustafa MS, Ramasethu R. Zika: An enormous public health challenge for a miniscule virus. Med J Armed Forces India [Internet]. 2018 Jan 1 [cited 2025 Jul 6];74(1):61–4. Available from: https://www.sciencedirect.com/science/article/pii/S0377123716301162
- Stark C, Sorensen I, Royall M. Maternal and Fetal Health Risks Among Female Military Aviation Officers. ingentaconnect.com [Internet]. [cited 2025 Jul 6]; Available from: https://www.ingentaconnect.com/content/asma/amhp/2024/00000095/00000009/art00009
- Virkutyte J, Slagley J, Miller ; Michael, Col L, Cooper C, Mbonimpa E, et al. Maternal Aircrew Fetal Noise and Vibration Exposure Risk Model. 2021 [cited 2025 Jul 6]; Available from: https://apps.dtic.mil/sti/html/trecms/AD1156332/
- Gender CGHarvJ&, 2022 undefined. Eliminating” Built-in Headwinds”: Strengthening the Military by Integrating the Condition of Pregnancy. HeinOnline [Internet]. [cited 2025 Jul 6]; Available from: https://heinonline.org/hol-cgi-bin/get_pdf.cgi?handle=hein.journals/hwlj45§ion=6
- Truijens SEM, Boerekamp CAM, Spek V, Van Son MJM, Oei SG, Pop VJM. Increased levels of depressive symptoms among pregnant women in The Netherlands after the crash of flight MH17. Am J Epidemiol. 2015 Sep 1;182(5):426–30.
- Tchirikov M, Oshovskyy V, Steetskamp J, Thäle V. Neonatal outcome following long-distance air travel for fetoscopic laser coagulation treatment of twin-to-twin transfusion syndrome. International Journal of Gynecology & Obstetrics. 2024 Jul;117:260–3.
- Petrikovsky B, Terrani M, Sichinava L. Transatlantic air travel in the third trimester of pregnancy: Does it affect the fetus? Am J Perinatol [Internet]. 2018 [cited 2025 Jul 5];8(2):E71–3. Available from: https://pubmed.ncbi.nlm.nih.gov/29670815/
- Grajewski B, Whelan E, Lawson C. Miscarriage among flight attendants. journals.lww.com [Internet]. [cited 2025 Jul 6]; Available from: https://journals.lww.com/epidem/fulltext/2015/03000/Miscarriage_Among_Flight_Attendants.11.aspx
- Ram HS, Ram S, Miller N, Rosental YS, Chodick G. Air travel during pregnancy and the risk of adverse pregnancy outcomes as gestational age and weight at birth: A retrospective study among 284,069 women in Israel. journals.plos.org [Internet]. 2020 Feb 1 [cited 2025 Jul 6];15(2). Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0228639
- Ram S, Shalev-Ram H, Neuhof B, Shlezinger R, Shalev-Rosental Y, Chodick G, et al. Air travel during pregnancy and the risk of venous thrombosis. Am J Obstet Gynecol MFM [Internet]. 2023 Jan 1 [cited 2025 Jul 6];5(1). Available from: https://www.sciencedirect.com/science/article/pii/S2589933322001823
- Heidecker B, Spencer RM, Hayes V, Hall S, Parikh N, Stock EO, et al. High Prevalence and Clinical/Sociodemographic Correlates of Miscarriages Among Flight Attendants. American Journal of Medicine [Internet]. 2017 Dec 1 [cited 2025 Jul 6];130(12):1397–401. Available from: https://www.sciencedirect.com/science/article/pii/S0002934317306113
- Aspholm R, Lindbohm ML, Paakkulainen H, Taskinen H, Nurminen T, Tiitinen A. Spontaneous Abortions Among Finnish Flight Attendants. J Occup Environ Med [Internet]. 1999;41(6). Available from: https://journals.lww.com/joem/fulltext/1999/06000/spontaneous_abortions_among_finnish_flight.15.aspx
- Fernando M, L. Giles M, Krishnaswamy S, Cole S. The pregnant traveller: An overview of general travel advice. Australian and New Zealand Journal of Obstetrics and Gynaecology. 2023 Oct 1;63(5):638–42.
- Magann EF, Chauhan SP, Dahlke JD, McKelvey SS, Watson EM, Morrison JC. Air Travel and Pregnancy Outcomes: A Review of Pregnancy Regulations and Outcomes for Passengers, Flight Attendants, and Aviators. Obstet Gynecol Surv. 2010 Jul;65:396–402.
- Beeton S. Pregnancy and travel. Community Nurse [Internet]. 1996;2:45–7. Available from: https://pubmed.ncbi.nlm.nih.gov/9450466/
- Walentiny C. [Pregnancy and traveling]. Dtsch Med Wochenschr [Internet]. 2009 Jul;134:594–8. Available from: https://pubmed.ncbi.nlm.nih.gov/19277936/
- Vethanayagam B, Kahn SR. Flying while pregnant: What is the thrombosis risk? Vol. 27, Journal of Travel Medicine. Oxford University Press; 2020.