Research
HJOG 2026, 25 (3), 190-197 | doi: 10.33574/hjog.0627
Muhammad Risal Djalika, Efendi Lukas, Sriwijaya Qadar, Firdaus Hamid, Ananda Mardiah Prefitri, Fatmawati Madya
Department of Obstetrics and Gynecology, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Correspondence: Muhammad Risal Djalika, Department of Obstetrics and Gynecology, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia, e-mail: risaldjalika@gmail.com
![]()
Abstract
Introduction: Preeclampsia is a major hypertensive disorder of pregnancy and a leading cause of maternal and perinatal morbidity and mortality worldwide. Kidney Injury Molecule-1 (KIM-1) has emerged as a promising biomarker of early renal tubular injury; however, its association with severe preeclampsia remains insufficiently established.
Material and methods: An analytic observational study with a cross-sectional design was conducted between June and December 2024 at Hasanuddin University Hospital, Makassar, Indonesia. A total of 105 pregnant women were enrolled, including 70 women with severe preeclampsia and 35 normotensive controls. Midstream urine samples were collected and urinary Kidney Injury Molecule-1 (KIM-1) levels were measured using enzyme-linked immunosorbent assay (ELISA). Comparisons between groups were performed using the Mann–Whitney U test and Kruskal–Wallis test, while correlations were assessed using Spearman’s rank correlation. A p-value <0.05 was considered statistically significant.
Results: Urinary KIM-1 levels were significantly higher in women with severe preeclampsia than in normotensive controls (median 2.03 [1.50–3.70] vs. 1.34 [0.60–1.53] ng/mL, p < 0.001). Urinary KIM-1 levels showed significant positive correlations with systolic blood pressure (r = 0.544, p < 0.001) and diastolic blood pressure (r = 0.447, p < 0.001). Higher urinary KIM-1 concentrations were also observed in overweight women (p = 0.033) and in preterm pregnancies (p = 0.020).
Conclusion: Urinary KIM-1 levels were significantly elevated in women with severe preeclampsia and were positively associated with blood pressure, suggesting that urinary KIM-1 may serve as a sensitive, non-invasive biomarker of early renal tubular injury in severe preeclampsia.
Key words: Severe preeclampsia, kidney Injury Molecule-1, urinary biomarker, renal tubular injury, hypertensive disorders of pregnancy
Introduction
Preeclampsia is a multisystem hypertensive disorder of pregnancy characterized by new-onset hypertension after 20 weeks of gestation, accompanied by proteinuria or evidence of maternal organ dysfunction. It remains one of the leading causes of maternal and perinatal morbidity and mortality worldwide, affecting approximately 2–8% of pregnancies. In Indonesia, preeclampsia continues to contribute substantially to maternal mortality despite advances in antenatal care. The condition is associated with serious maternal complications, including eclampsia, stroke, acute kidney injury, hepatic dysfunction, and disseminated intravascular coagulation, as well as adverse fetal outcomes such as fetal growth restriction, preterm birth, and perinatal death1-3.
The pathogenesis of preeclampsia is complex and involves abnormal placentation, inadequate trophoblastic invasion, and impaired remodeling of the spiral arteries. These abnormalities result in placental ischemia, oxidative stress, and the release of antiangiogenic and inflammatory mediators into the maternal circulation, leading to widespread endothelial dysfunction. The kidneys are among the organs most frequently affected, with renal involvement characterized by glomerular endotheliosis, reduced glomerular filtration rate, and tubular epithelial injury. Although serum creatinine and blood urea nitrogen are routinely used to evaluate renal function, these conventional biomarkers often remain within the normal range until significant renal impairment has occurred, limiting their usefulness for detecting early kidney injury4-9.
Kidney Injury Molecule-1 (KIM-1) is a type I transmembrane glycoprotein that is minimally expressed in healthy kidneys but markedly upregulated in proximal tubular epithelial cells following ischemic or toxic injury. After tubular damage, the extracellular domain of KIM-1 is shed into the urine, making it a sensitive and non-invasive biomarker for early renal tubular injury.
Previous studies have demonstrated significantly higher urinary KIM-1 levels in women with preeclampsia than in normotensive pregnancies, suggesting that KIM-1 may identify renal injury before abnormalities in conventional renal function tests become evident. Furthermore, urinary KIM-1 has been associated with disease severity and adverse maternal outcomes, highlighting its potential clinical value in hypertensive disorders of pregnancy10-16.
Despite growing evidence supporting the diagnostic value of urinary KIM-1, data from Southeast Asian populations remain limited, and its relationship with clinical indicators of disease severity has not been adequately investigated. Evaluating urinary KIM-1 levels in women with severe preeclampsia may improve understanding of renal involvement and facilitate earlier identification of subclinical kidney injury.
Therefore, this study aimed to compare urinary Kidney Injury Molecule-1 (KIM-1) levels between women with severe preeclampsia and normotensive pregnancies and to evaluate the association between urinary KIM-1 levels and clinical parameters of disease severity.
Material and methods
Study Design and Setting
This analytic observational study employed a cross-sectional design and was conducted at the Department of Obstetrics and Gynecology, Hasanuddin University Hospital, Makassar, Indonesia, from June to December 2024. The study aimed to compare urinary Kidney Injury Molecule-1 (KIM-1) levels between women with severe preeclampsia and normotensive pregnant women and to evaluate the association between urinary KIM-1 levels and clinical indicators of disease severity.
Study Population
Pregnant women attending Hasanuddin University Hospital during the study period were consecutively recruited. A total of 105 participants were included in the study, comprising 70 women with severe preeclampsia and 35 normotensive pregnant women who served as the control group.
Severe preeclampsia was diagnosed according to the American College of Obstetricians and Gynecologists (ACOG) Practice Bulletin No. 222 (2020), defined as new-onset hypertension after 20 weeks of gestation (systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg) accompanied by proteinuria or evidence of maternal end-organ dysfunction.
Inclusion and Exclusion Criteria
Eligible participants were women aged ≥18 years with singleton pregnancies of at least 20 weeks’ gestation who provided written informed consent.
Women with chronic kidney disease, chronic hypertension, diabetes mellitus, urinary tract infection, autoimmune disorders, multiple pregnancy, congenital renal abnormalities, or incomplete clinical and laboratory data were excluded.
Sample Collection and Measurement of Urinary KIM-1
Approximately 10 mL of midstream urine was collected from each participant under aseptic conditions before delivery. The urine samples were centrifuged at 3,000 rpm for 10 minutes, and the supernatant was aliquoted and stored at −20°C until laboratory analysis.
Urinary KIM-1 concentrations were determined using a commercially available enzyme-linked immunosorbent assay (ELISA) kit according to the manufacturer’s instructions. (Human KIM-1 ELISA Kit, BT Lab, Shaghai, China; Cat. No. E1099Hu)
Maternal demographic characteristics, body mass index (BMI), parity, gestational age, systolic blood pressure, diastolic blood pressure, serum urea, serum creatinine, and urinary KIM-1 concentrations were collected from clinical examinations and medical records.
Ethical Considerations
The study protocol was approved by the Health Research Ethics Committee, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia (Approval No. 27/ UN4.6.4.5.31 / PP36 / 2025). Written informed consent was obtained from all participants before enrollment. All procedures were conducted in accordance with the ethical principles of the Declaration of Helsinki (2013).
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics version 27.0 (IBM Corp., Armonk, NY, USA).
Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed data are presented as mean ± standard deviation (SD), whereas non-normally distributed data are presented as median (interquartile range [IQR]). Categorical variables are expressed as frequencies and percentages.
Comparisons between the severe preeclampsia and control groups were performed using the independent-samples t-test for normally distributed variables or the Mann–Whitney U test for non-normally distributed variables. Comparisons among more than two groups were analyzed using the Kruskal–Wallis test. Correlations between urinary KIM-1 levels and continuous clinical variables were assessed using Spearman’s rank correlation coefficient. A two-tailed p-value <0.05 was considered statistically significant.
Results
A total of 105 pregnant women who met the inclusion and exclusion criteria were enrolled in this study. The study population consisted of 70 women with severe preeclampsia and 35 normotensive pregnant women.
Baseline Characteristics
The baseline demographic and clinical characteristics of the participants are presented in Table 1. Most participants were aged 20–35 years (82.9%), were multigravida (61.9%), and had term pregnancies (88.6%).
No significant differences were observed between the severe preeclampsia and control groups regarding maternal age, parity, or gestational age (all p >0.05). However, body mass index (BMI) differed significantly between the two groups (p =0.001), with obesity being more prevalent among women with severe preeclampsia. Although serum urea and creatinine levels were higher in the severe preeclampsia group, these differences were not statistically significant.
Comparison of Urinary KIM-1 Levels
The comparison of urinary KIM-1 concentrations between the study groups is presented in Table 2 and Figure 1.
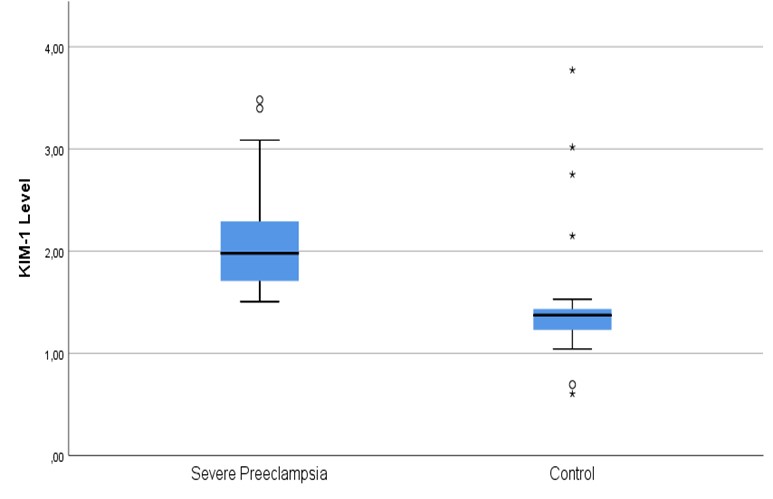
Figure 1. Boxplot showing the distribution of urinary Kidney Injury Molecule-1 (KIM-1) levels in women with severe preeclampsia and normotensive pregnancies. Women with severe preeclampsia had significantly higher urinary KIM-1 levels than normotensive controls. Description: Mann–Whitney U test, p < 0.001.
Women with severe preeclampsia had significantly higher urinary KIM-1 levels than normotensive controls (median 2.03 [1.50–3.70] ng/mL vs. 1.34 [0.60–1.53] ng/mL, p <0.001).
Association Between Urinary KIM-1 Levels and Maternal Characteristics
The relationship between urinary KIM-1 levels and maternal characteristics is shown in Table 3.
Urinary KIM-1 concentrations differed significantly according to maternal BMI (p =0.033), with the highest levels observed among overweight women. In addition, urinary KIM-1 levels were significantly higher in preterm pregnancies than in term pregnancies (p =0.020).
Correlation Between Urinary KIM-1 Levels and Blood Pressure
The correlations between urinary KIM-1 levels and maternal blood pressure are illustrated in Figure 2.
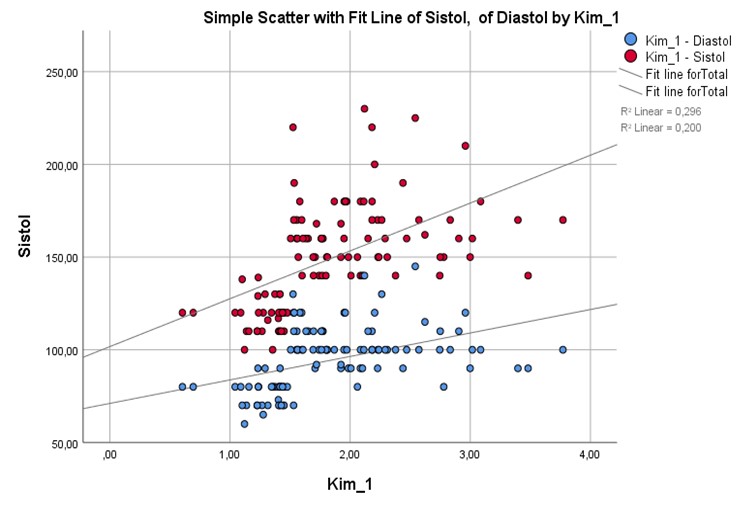
Figure 2. Scatter plots demonstrating the correlations between urinary KIM-1 levels and systolic (A) and diastolic (B) blood pressure in women with severe preeclampsia.
Spearman’s correlation analysis demonstrated a moderate positive correlation between urinary KIM-1 levels and systolic blood pressure (r =0.544, p <0.001). A moderate positive correlation was also observed between urinary KIM-1 levels and diastolic blood pressure (r =0.447, p <0.001).
Discussion
This study demonstrated that urinary Kidney Injury Molecule-1 (KIM-1) levels were significantly higher in women with severe preeclampsia than in normotensive pregnancies. Furthermore, urinary KIM-1 levels showed significant positive correlations with systolic and diastolic blood pressure and were associated with maternal body mass index and gestational age. These findings support the hypothesis that renal tubular injury occurs in severe preeclampsia and that urinary KIM-1 may serve as a sensitive biomarker of early renal involvement.
The present findings are consistent with previous studies reporting elevated urinary KIM-1 concentrations in women with preeclampsia. Moresco et al. demonstrated that urinary KIM-1 levels were significantly increased in hypertensive disorders of pregnancy compared with normotensive pregnancies, indicating that tubular epithelial injury develops early during disease progression. Likewise, Ramdin et al. reported that urinary KIM-1 exhibited promising diagnostic performance for identifying renal injury in women with preeclampsia. Kamel et al. further suggested that urinary KIM-1 reflects proximal tubular injury and may provide additional information beyond conventional renal function tests. Collectively, these findings support the potential role of urinary KIM-1 as an early biomarker of kidney injury in hypertensive disorders of pregnancy.
The biological mechanism underlying elevated urinary KIM-1 levels in severe preeclampsia is closely related to placental ischemia and systemic endothelial dysfunction. Inadequate trophoblastic invasion and impaired remodeling of the spiral arteries lead to placental hypoperfusion and oxidative stress, resulting in the release of inflammatory cytokines and antiangiogenic factors into the maternal circulation. These mediators impair renal microvascular perfusion and induce ischemic injury of proximal tubular epithelial cells. Under these conditions, KIM-1 expression is markedly upregulated, and its extracellular domain is shed into the urine, making it a sensitive indicator of ongoing tubular injury before conventional renal function markers become abnormal.
In this study, urinary KIM-1 levels were positively correlated with both systolic and diastolic blood pressure, suggesting that greater hypertension is associated with more pronounced renal tubular injury. Increasing blood pressure may aggravate renal ischemia through endothelial dysfunction and altered renal hemodynamics, thereby promoting tubular epithelial damage. Higher urinary KIM-1 concentrations were also observed among overweight women and in preterm pregnancies, indicating that maternal metabolic status and earlier disease onset may contribute to greater renal injury. Obesity is recognized as a pro-inflammatory condition characterized by chronic low-grade inflammation and oxidative stress, both of which may exacerbate endothelial dysfunction in preeclampsia. Similarly, preterm preeclampsia is generally associated with more severe placental dysfunction and systemic maternal disease than term preeclampsia.
An important finding of the present study is that urinary KIM-1 levels were elevated despite the absence of significant differences in conventional renal biomarkers, namely serum urea and creatinine. This observation suggests that tubular injury may precede detectable impairment of glomerular filtration, highlighting the greater sensitivity of urinary KIM-1 for identifying early renal involvement. Therefore, urinary KIM-1 may complement conventional laboratory tests by detecting subclinical kidney injury before irreversible renal dysfunction develops.
The present study has several strengths. First, it evaluated urinary KIM-1 as a non-invasive biomarker in women with severe preeclampsia using a standardized ELISA method. Second, correlations between urinary KIM-1 and multiple clinical parameters were analyzed, providing additional evidence regarding its clinical relevance. Nevertheless, several limitations should be acknowledged. The cross-sectional design precludes causal inference, the study was conducted at a single tertiary referral center, and the sample size was relatively modest. Furthermore, only urinary KIM-1 was evaluated without comparison with other emerging renal biomarkers such as neutrophil gelatinase-associated lipocalin (NGAL) or cystatin C.
Overall, the findings indicate that urinary KIM-1 is significantly associated with severe preeclampsia and clinical indicators of disease severity. Measurement of urinary KIM-1 may improve the early identification of renal tubular injury and contribute to risk stratification in women with severe preeclampsia. Future multicenter prospective studies with larger populations are warranted to validate these findings and determine clinically applicable diagnostic cut-off values.
Conclusion
Urinary Kidney Injury Molecule-1 (KIM-1) levels were significantly higher in women with severe preeclampsia than in normotensive pregnancies and were positively associated with systolic and diastolic blood pressure. These findings indicate that urinary KIM-1 is associated with renal tubular injury and disease severity in severe preeclampsia. As a non-invasive biomarker, urinary KIM-1 may complement conventional renal function tests by facilitating the early detection of renal involvement. Further prospective multicenter studies with larger sample sizes are warranted to validate its diagnostic and prognostic value in clinical practice.
Conflict of Interest
The authors declare that they have no conflicts of interest related to this study.
References
- Basyiar A, Fitriani V, Rizki M, Arifin H. The relationship between obesity and preeclampsia in pregnant women. BMC Pregnancy Childbirth. 2021;21(1):210.
- Khedagi AM, Bello NA. Preeclampsia: Pathophysiology and clinical presentation with cardiovascular implications. Cardiol Clin. 2021;39(1):15–23.
- Ministry of Health of the Republic of Indonesia. Indonesia Health Profile 2017. Jakarta: Ministry of Health of the Republic of Indonesia; 2018.
- Granger JP, Alexander BT, Llinas MT, Bennett WA, Khalil RA. Pathophysiology of hypertension during preeclampsia: Linking placental ischemia with endothelial dysfunction. Hypertension. 2001;38(3 Pt 2):718–22.
- Staff AC, Fjeldstad HE, Fosheim IK, Moe K, Turowski G, Johnsen GM, et al. Failure of spiral artery remodeling in the placenta: A link to preeclampsia. Am J Obstet Gynecol. 2013;209(6):569–76.
- Tannetta DS, Sargent IL. Placental syncytiotrophoblast vesicles: Circulating biopsies reflecting placental health. Placenta. 2013;34(Suppl 1)–13.
- Garovic VD, Wagner SJ, Petrovic LM, Gray CE, Hall P, Sugimoto H, et al. Glomerular endotheliosis is a renal lesion characteristic of preeclampsia and not of pregnancy alone. Am J Kidney Dis. 2007;50(5):865–72.
- Wang A, Rana S, Karumanchi SA. Preeclampsia: The role of angiogenic factors in its pathogenesis. Physiology (Bethesda). 2015;30(3):147–58.
- Xiao J, Niu J, Ye X, Yu Q, Gu Y. Systemic endothelial dysfunction in preeclampsia: From bench to bedside. Am J Physiol Heart Circ Physiol. 2013;305(4)–58.
- Cai L, Rubera I, Roussel D, N’Guessan P, Goujon JM, Nivet H, et al. The use of kidney injury molecule-1 (KIM-1) as a sensitive and specific biomarker of kidney injury in humans and animals. Clin Chim Acta. 2019;498:80–91.
- Moresco RN, Bochi GV, Stein CS, De Carvalho JAM, Cembranel BM, Bollick YS. Urinary kidney injury molecule-1 in hypertensive disorders of pregnancy. Clin Chim Acta. 2018;478:111–6.
- Ramdin T, Govender S, Moodley J, Naicker T. Urinary kidney injury molecule-1 as a diagnostic marker of preeclampsia. Pregnancy Hypertens. 2023;31:31–7.
- Belcher JM, Parikh CR, Garcia-Tsao G. Acute kidney injury in cirrhosis: Prevention and therapy. Curr Opin Crit Care. 2014;20(6):612–9.
- Kamel KS, Halim MA, Farouk N, Saleh S, Mostafa H. Role of urinary kidney injury molecule-1 (KIM-1) in prediction of renal involvement in preeclampsia. Egypt J Intern Med. 2020;32(1):1–7.
- Burwick RM, Feinberg BB, Egan BM. The complement system and preeclampsia: New insights into an old disease. Am J Reprod Immunol. 2014;72(5):395–403.
- Mose FH, Moller HJ, Lindhardt JM, Frøkiær J, Flyvbjerg A. Kidney injury molecule-1 and neutrophil gelatinase-associated lipocalin in preeclampsia. Pregnancy Hypertens. 2019;18:32–8.
- Redman CW, Sargent IL. Latest advances in understanding preeclampsia. Science. 2005;308(5728):1592–4.
- Gist KM, Faubel S, Knapp KM, Goldstein SL. Serum and urine biomarkers for acute kidney injury: Where are we now? Adv Chronic Kidney Dis. 2018;25(3):251–62.